Lucia Introini, Jenifer Silva, Mariana Risso, Beatriz Mendoza, Maria M Pineyro
{"title":"妊娠期垂体瘤卒中伴微泌乳素瘤生长:病例报告及文献复习。","authors":"Lucia Introini, Jenifer Silva, Mariana Risso, Beatriz Mendoza, Maria M Pineyro","doi":"10.1155/crie/2490132","DOIUrl":null,"url":null,"abstract":"<p><p>Prolactinomas are the most prevalent subtype of pituitary adenomas and represent one of the leading etiological factors responsible for amenorrhea and infertility in women. The primary therapeutic approach entails the use of dopamine agonists, which effectively restore fertility. In cases of microprolactinomas, the likelihood of experiencing a symptomatic enlargement of the tumor during pregnancy is exceptionally low, estimated at a mere 2.4%. Consequently, once pregnancy is successfully achieved, the administration of dopamine agonists is discontinued, with ongoing clinical monitoring of the patient's condition. The incidence of pituitary apoplexy during pregnancy is exceedingly rare. We present a case of a 29-year-old patient with microprolactinoma, treated with cabergoline, which was discontinued upon achieving pregnancy. However, at the 16th week of gestation, she presented with persistent headaches and compromised visual acuity, manifesting as left temporal hemianopia. A noncontrast magnetic resonance imaging (MRI) revealed an enlargement of the adenoma, accompanied by evidence of hemorrhage. She was referred to our hospital at 26 weeks of gestation. Cabergoline treatment was reinstated and well tolerated by the patient. Doses were increased to 2 mg per week because bitemporal hemianopia was not improving. A subsequent noncontrast MRI scan performed at 35 weeks of gestation demonstrated a further increase in adenoma size, measuring 17 × 21 × 13 mm, with signs of intratumoral bleeding. A planned cesarean section was performed at 39 weeks of gestation, without encountering maternal-fetal complications. Breastfeeding was not initiated due to the adenoma's compression of the chiasm. Accordingly, dopamine agonist therapy was continued. During the postpartum follow-up, the patient experienced a resumption of menstrual cycles, normalization of prolactin levels, and a reduction in tumor size. Ultimately, the diagnosis was established as a microprolactinoma, which had enlarged during pregnancy due to a pituitary tumor apoplexy. Although microprolactinomas typically carry a low risk of symptomatic tumor growth during pregnancy, this case emphasizes the critical importance of vigilant clinical monitoring to swiftly detect and manage this rare complication. This instance serves as an educational example of an uncommon event-a microprolactinoma experiencing apoplexy during pregnancy.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2025 ","pages":"2490132"},"PeriodicalIF":0.9000,"publicationDate":"2025-01-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732282/pdf/","citationCount":"0","resultStr":"{\"title\":\"Microprolactinoma Growth During Pregnancy With Pituitary Tumor Apoplexy: Case Report and Review of the Literature.\",\"authors\":\"Lucia Introini, Jenifer Silva, Mariana Risso, Beatriz Mendoza, Maria M Pineyro\",\"doi\":\"10.1155/crie/2490132\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Prolactinomas are the most prevalent subtype of pituitary adenomas and represent one of the leading etiological factors responsible for amenorrhea and infertility in women. The primary therapeutic approach entails the use of dopamine agonists, which effectively restore fertility. In cases of microprolactinomas, the likelihood of experiencing a symptomatic enlargement of the tumor during pregnancy is exceptionally low, estimated at a mere 2.4%. Consequently, once pregnancy is successfully achieved, the administration of dopamine agonists is discontinued, with ongoing clinical monitoring of the patient's condition. The incidence of pituitary apoplexy during pregnancy is exceedingly rare. We present a case of a 29-year-old patient with microprolactinoma, treated with cabergoline, which was discontinued upon achieving pregnancy. However, at the 16th week of gestation, she presented with persistent headaches and compromised visual acuity, manifesting as left temporal hemianopia. A noncontrast magnetic resonance imaging (MRI) revealed an enlargement of the adenoma, accompanied by evidence of hemorrhage. She was referred to our hospital at 26 weeks of gestation. Cabergoline treatment was reinstated and well tolerated by the patient. Doses were increased to 2 mg per week because bitemporal hemianopia was not improving. A subsequent noncontrast MRI scan performed at 35 weeks of gestation demonstrated a further increase in adenoma size, measuring 17 × 21 × 13 mm, with signs of intratumoral bleeding. A planned cesarean section was performed at 39 weeks of gestation, without encountering maternal-fetal complications. Breastfeeding was not initiated due to the adenoma's compression of the chiasm. Accordingly, dopamine agonist therapy was continued. During the postpartum follow-up, the patient experienced a resumption of menstrual cycles, normalization of prolactin levels, and a reduction in tumor size. Ultimately, the diagnosis was established as a microprolactinoma, which had enlarged during pregnancy due to a pituitary tumor apoplexy. Although microprolactinomas typically carry a low risk of symptomatic tumor growth during pregnancy, this case emphasizes the critical importance of vigilant clinical monitoring to swiftly detect and manage this rare complication. This instance serves as an educational example of an uncommon event-a microprolactinoma experiencing apoplexy during pregnancy.</p>\",\"PeriodicalId\":9621,\"journal\":{\"name\":\"Case Reports in Endocrinology\",\"volume\":\"2025 \",\"pages\":\"2490132\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-01-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732282/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crie/2490132\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crie/2490132","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Microprolactinoma Growth During Pregnancy With Pituitary Tumor Apoplexy: Case Report and Review of the Literature.
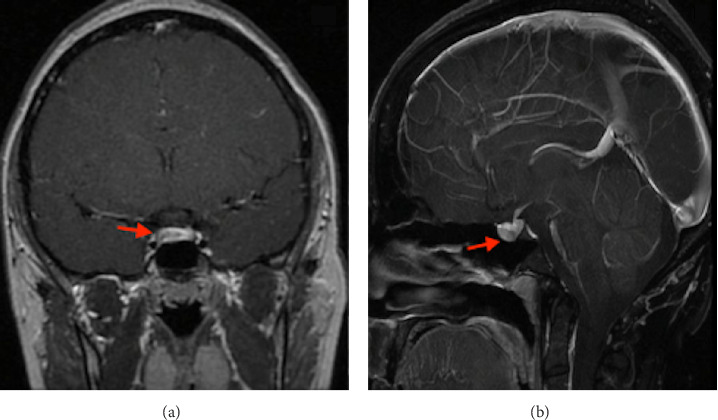
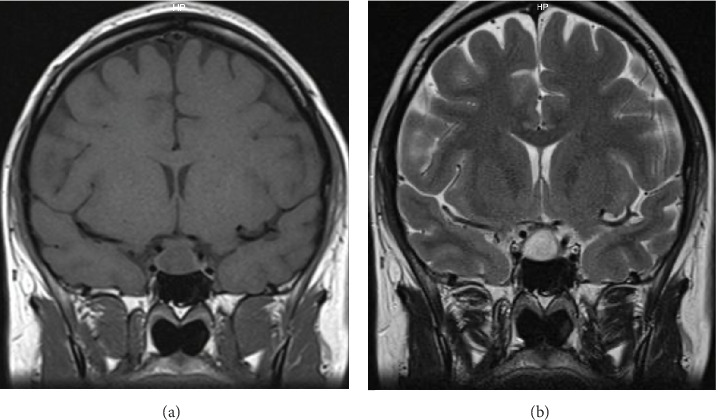
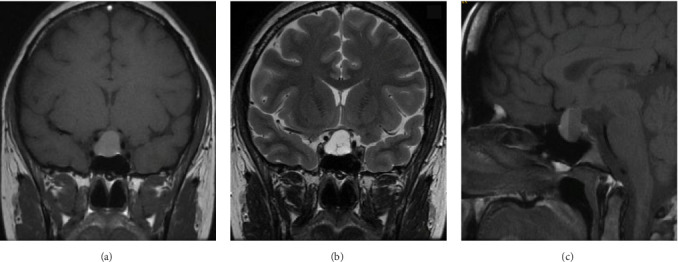
Prolactinomas are the most prevalent subtype of pituitary adenomas and represent one of the leading etiological factors responsible for amenorrhea and infertility in women. The primary therapeutic approach entails the use of dopamine agonists, which effectively restore fertility. In cases of microprolactinomas, the likelihood of experiencing a symptomatic enlargement of the tumor during pregnancy is exceptionally low, estimated at a mere 2.4%. Consequently, once pregnancy is successfully achieved, the administration of dopamine agonists is discontinued, with ongoing clinical monitoring of the patient's condition. The incidence of pituitary apoplexy during pregnancy is exceedingly rare. We present a case of a 29-year-old patient with microprolactinoma, treated with cabergoline, which was discontinued upon achieving pregnancy. However, at the 16th week of gestation, she presented with persistent headaches and compromised visual acuity, manifesting as left temporal hemianopia. A noncontrast magnetic resonance imaging (MRI) revealed an enlargement of the adenoma, accompanied by evidence of hemorrhage. She was referred to our hospital at 26 weeks of gestation. Cabergoline treatment was reinstated and well tolerated by the patient. Doses were increased to 2 mg per week because bitemporal hemianopia was not improving. A subsequent noncontrast MRI scan performed at 35 weeks of gestation demonstrated a further increase in adenoma size, measuring 17 × 21 × 13 mm, with signs of intratumoral bleeding. A planned cesarean section was performed at 39 weeks of gestation, without encountering maternal-fetal complications. Breastfeeding was not initiated due to the adenoma's compression of the chiasm. Accordingly, dopamine agonist therapy was continued. During the postpartum follow-up, the patient experienced a resumption of menstrual cycles, normalization of prolactin levels, and a reduction in tumor size. Ultimately, the diagnosis was established as a microprolactinoma, which had enlarged during pregnancy due to a pituitary tumor apoplexy. Although microprolactinomas typically carry a low risk of symptomatic tumor growth during pregnancy, this case emphasizes the critical importance of vigilant clinical monitoring to swiftly detect and manage this rare complication. This instance serves as an educational example of an uncommon event-a microprolactinoma experiencing apoplexy during pregnancy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
