{"title":"一项回顾性队列研究:bbbb2cm磨玻璃样混浊非小细胞肺癌的T期分级策略的验证。","authors":"Yiming Li, Zhenyu Yang, Hui Jie, Liying Zhang, Chenglin Guo, Chengwu Liu, Qiang Pu, Lunxu Liu","doi":"10.21037/tlcr-24-664","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Lung Cancer Staging Program of the International Association for the Study of Lung Cancer (IASLC) has proposed using solid component size, rather than overall tumor size, for T-staging. However, studies focusing on patients with ground-glass opacity (GGO) lesions with a diameter larger than 2 cm are limited. This study aims to validate the T stage classification strategy recommended by IASLC in this specific and less-studied patient group.</p><p><strong>Methods: </strong>Patients diagnosed with primary non-small cell lung cancer (NSCLC) who underwent lobectomy between December 2009 and December 2018 were included in this study. Clinical, pathological, and prognostic data were prospectively collected and retrospectively reviewed. Patients were eligible if they were confirmed to have NSCLC, underwent lobectomy, had complete follow-up data, and were not diagnosed with any other malignancies. The propensity score matching (PSM) method was employed to ensure baseline characteristic balance. Two groups of patients matched with the GGO group at baseline were stratified based on overall tumor size (group matched by overall size) and solid component size (group matched by solid component size), respectively. Overall survival (OS) and recurrence-free survival (RFS) were analyzed using the Cox proportional model and Kaplan-Meier method. Follow-up was conducted regularly to assess these outcomes. The T-staging applied was based on the solid component size according to the 8th edition IASLC staging guidelines.</p><p><strong>Results: </strong>A total of 4,472 NSCLC patients who underwent lobectomy were included in the study (including 4,083 cases of solid lesions and 389 cases of subsolid lesions). The median follow-up time was 75.4 months. Patients in the GGO group had significantly better OS and RFS than those in the solid group [OS: hazard ratio (HR) =0.55, 95% confidence interval (CI): 0.40-0.73, P<0.001; RFS: HR =0.53, 95% CI: 0.42-0.67, P<0.001]. Comparing patients' PSM by overall size, the GGO group still had better OS and RFS (OS: HR =0.60, 95% CI: 0.43-0.85, P=0.004; RFS: HR =0.59, 95% CI: 0.44-0.79, P<0.001). After PSM by solid component size, no significant difference was detected between the GGO group and the group matched by solid component size on OS and RFS (OS: HR =0.89, 95% CI: 0.61-1.28, P=0.52; RFS: HR =0.92, 95% CI: 0.67-1.26, P=0.61). In subgroup analysis, after PSM by solid component size, the results showed no difference in OS and RFS between the restaged patients (c-T1 and c-T2) and the corresponding patients in the solid group (for OS, HR =1.06, 95% CI: 0.61-1.83, P=0.83; HR =1.11, 95% CI: 0.60-2.07, P=0.73, respectively; and RFS, HR =1.17, 95% CI: 0.75-1.82, P=0.49; HR =0.80, 95% CI: 0.48-1.34, P=0.39, respectively).</p><p><strong>Conclusions: </strong>The T stage classification strategy proposed by ISALC remains applicable in patients with GGOs larger than 2 cm.</p>","PeriodicalId":23271,"journal":{"name":"Translational lung cancer research","volume":"13 12","pages":"3526-3537"},"PeriodicalIF":3.4000,"publicationDate":"2024-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11736582/pdf/","citationCount":"0","resultStr":"{\"title\":\"Validation of T stage classification strategy for >2 cm ground-glass opacity non-small cell lung cancer: a retrospective cohort study.\",\"authors\":\"Yiming Li, Zhenyu Yang, Hui Jie, Liying Zhang, Chenglin Guo, Chengwu Liu, Qiang Pu, Lunxu Liu\",\"doi\":\"10.21037/tlcr-24-664\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Lung Cancer Staging Program of the International Association for the Study of Lung Cancer (IASLC) has proposed using solid component size, rather than overall tumor size, for T-staging. However, studies focusing on patients with ground-glass opacity (GGO) lesions with a diameter larger than 2 cm are limited. This study aims to validate the T stage classification strategy recommended by IASLC in this specific and less-studied patient group.</p><p><strong>Methods: </strong>Patients diagnosed with primary non-small cell lung cancer (NSCLC) who underwent lobectomy between December 2009 and December 2018 were included in this study. Clinical, pathological, and prognostic data were prospectively collected and retrospectively reviewed. Patients were eligible if they were confirmed to have NSCLC, underwent lobectomy, had complete follow-up data, and were not diagnosed with any other malignancies. The propensity score matching (PSM) method was employed to ensure baseline characteristic balance. Two groups of patients matched with the GGO group at baseline were stratified based on overall tumor size (group matched by overall size) and solid component size (group matched by solid component size), respectively. Overall survival (OS) and recurrence-free survival (RFS) were analyzed using the Cox proportional model and Kaplan-Meier method. Follow-up was conducted regularly to assess these outcomes. The T-staging applied was based on the solid component size according to the 8th edition IASLC staging guidelines.</p><p><strong>Results: </strong>A total of 4,472 NSCLC patients who underwent lobectomy were included in the study (including 4,083 cases of solid lesions and 389 cases of subsolid lesions). The median follow-up time was 75.4 months. Patients in the GGO group had significantly better OS and RFS than those in the solid group [OS: hazard ratio (HR) =0.55, 95% confidence interval (CI): 0.40-0.73, P<0.001; RFS: HR =0.53, 95% CI: 0.42-0.67, P<0.001]. Comparing patients' PSM by overall size, the GGO group still had better OS and RFS (OS: HR =0.60, 95% CI: 0.43-0.85, P=0.004; RFS: HR =0.59, 95% CI: 0.44-0.79, P<0.001). After PSM by solid component size, no significant difference was detected between the GGO group and the group matched by solid component size on OS and RFS (OS: HR =0.89, 95% CI: 0.61-1.28, P=0.52; RFS: HR =0.92, 95% CI: 0.67-1.26, P=0.61). In subgroup analysis, after PSM by solid component size, the results showed no difference in OS and RFS between the restaged patients (c-T1 and c-T2) and the corresponding patients in the solid group (for OS, HR =1.06, 95% CI: 0.61-1.83, P=0.83; HR =1.11, 95% CI: 0.60-2.07, P=0.73, respectively; and RFS, HR =1.17, 95% CI: 0.75-1.82, P=0.49; HR =0.80, 95% CI: 0.48-1.34, P=0.39, respectively).</p><p><strong>Conclusions: </strong>The T stage classification strategy proposed by ISALC remains applicable in patients with GGOs larger than 2 cm.</p>\",\"PeriodicalId\":23271,\"journal\":{\"name\":\"Translational lung cancer research\",\"volume\":\"13 12\",\"pages\":\"3526-3537\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-12-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11736582/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational lung cancer research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/tlcr-24-664\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational lung cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tlcr-24-664","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Validation of T stage classification strategy for >2 cm ground-glass opacity non-small cell lung cancer: a retrospective cohort study.
Background: The Lung Cancer Staging Program of the International Association for the Study of Lung Cancer (IASLC) has proposed using solid component size, rather than overall tumor size, for T-staging. However, studies focusing on patients with ground-glass opacity (GGO) lesions with a diameter larger than 2 cm are limited. This study aims to validate the T stage classification strategy recommended by IASLC in this specific and less-studied patient group.
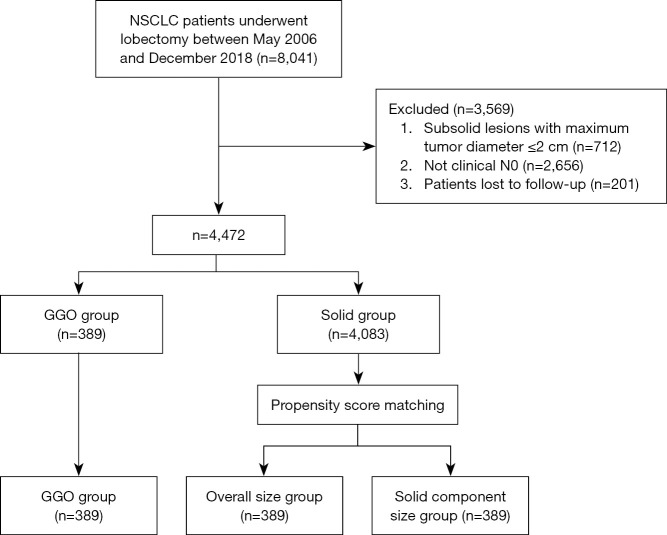
Methods: Patients diagnosed with primary non-small cell lung cancer (NSCLC) who underwent lobectomy between December 2009 and December 2018 were included in this study. Clinical, pathological, and prognostic data were prospectively collected and retrospectively reviewed. Patients were eligible if they were confirmed to have NSCLC, underwent lobectomy, had complete follow-up data, and were not diagnosed with any other malignancies. The propensity score matching (PSM) method was employed to ensure baseline characteristic balance. Two groups of patients matched with the GGO group at baseline were stratified based on overall tumor size (group matched by overall size) and solid component size (group matched by solid component size), respectively. Overall survival (OS) and recurrence-free survival (RFS) were analyzed using the Cox proportional model and Kaplan-Meier method. Follow-up was conducted regularly to assess these outcomes. The T-staging applied was based on the solid component size according to the 8th edition IASLC staging guidelines.
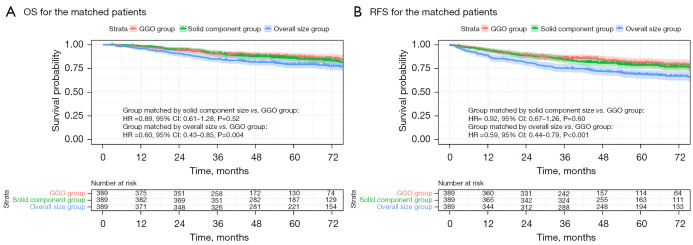
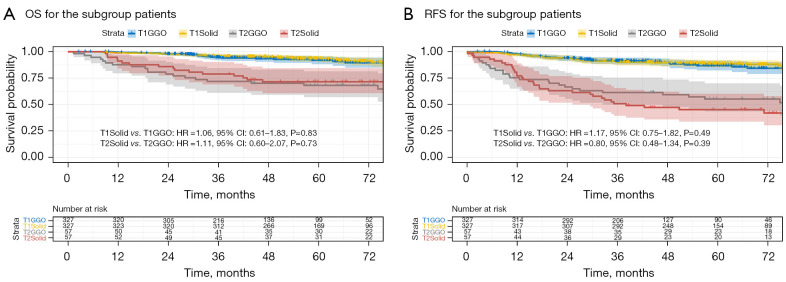
Results: A total of 4,472 NSCLC patients who underwent lobectomy were included in the study (including 4,083 cases of solid lesions and 389 cases of subsolid lesions). The median follow-up time was 75.4 months. Patients in the GGO group had significantly better OS and RFS than those in the solid group [OS: hazard ratio (HR) =0.55, 95% confidence interval (CI): 0.40-0.73, P<0.001; RFS: HR =0.53, 95% CI: 0.42-0.67, P<0.001]. Comparing patients' PSM by overall size, the GGO group still had better OS and RFS (OS: HR =0.60, 95% CI: 0.43-0.85, P=0.004; RFS: HR =0.59, 95% CI: 0.44-0.79, P<0.001). After PSM by solid component size, no significant difference was detected between the GGO group and the group matched by solid component size on OS and RFS (OS: HR =0.89, 95% CI: 0.61-1.28, P=0.52; RFS: HR =0.92, 95% CI: 0.67-1.26, P=0.61). In subgroup analysis, after PSM by solid component size, the results showed no difference in OS and RFS between the restaged patients (c-T1 and c-T2) and the corresponding patients in the solid group (for OS, HR =1.06, 95% CI: 0.61-1.83, P=0.83; HR =1.11, 95% CI: 0.60-2.07, P=0.73, respectively; and RFS, HR =1.17, 95% CI: 0.75-1.82, P=0.49; HR =0.80, 95% CI: 0.48-1.34, P=0.39, respectively).
Conclusions: The T stage classification strategy proposed by ISALC remains applicable in patients with GGOs larger than 2 cm.
期刊介绍:
Translational Lung Cancer Research(TLCR, Transl Lung Cancer Res, Print ISSN 2218-6751; Online ISSN 2226-4477) is an international, peer-reviewed, open-access journal, which was founded in March 2012. TLCR is indexed by PubMed/PubMed Central and the Chemical Abstracts Service (CAS) Databases. It is published quarterly the first year, and published bimonthly since February 2013. It provides practical up-to-date information on prevention, early detection, diagnosis, and treatment of lung cancer. Specific areas of its interest include, but not limited to, multimodality therapy, markers, imaging, tumor biology, pathology, chemoprevention, and technical advances related to lung cancer.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
