Maria Fleseriu, Richard J Auchus, Irina Bancos, Beverly M K Biller
{"title":"奥西洛德司他治疗肾上腺和异位库欣综合征:临床研究与病例介绍相结合。","authors":"Maria Fleseriu, Richard J Auchus, Irina Bancos, Beverly M K Biller","doi":"10.1210/jendso/bvaf027","DOIUrl":null,"url":null,"abstract":"<p><p>Although most cases of endogenous Cushing syndrome are caused by a pituitary adenoma (Cushing disease), approximately one-third of patients present with ectopic or adrenal causes. Surgery is the first-line treatment for most patients with Cushing syndrome; however, medical therapy is an important management option for those who are not eligible for, refuse, or do not respond to surgery. Clinical experience demonstrating that osilodrostat, an oral 11β-hydroxylase inhibitor, is effective and well tolerated comes predominantly from phase III trials in patients with Cushing disease. Nonetheless, reports of its use in patients with ectopic or adrenal Cushing syndrome are increasing. These data highlight the importance of selecting the most appropriate starting dose and titration frequency while monitoring for adverse events, including those related to hypocortisolism and prolongation of the QT interval, to optimize treatment outcomes. Here we use illustrative case studies to discuss practical considerations for the management of patients with ectopic or adrenal Cushing syndrome and review published data on the use of osilodrostat in these patients. The case studies show that to achieve the goal of reducing cortisol levels in all etiologies of Cushing syndrome, management should be individualized according to each patient's disease severity, comorbidities, performance status, and response to treatment. This approach to osilodrostat treatment maximizes the benefits of effective cortisol control, leads to improvements in comorbid conditions, and may ameliorate quality of life for patients across all types and severities of Cushing syndrome.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"9 4","pages":"bvaf027"},"PeriodicalIF":3.1000,"publicationDate":"2025-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915091/pdf/","citationCount":"0","resultStr":"{\"title\":\"Osilodrostat Treatment for Adrenal and Ectopic Cushing Syndrome: Integration of Clinical Studies With Case Presentations.\",\"authors\":\"Maria Fleseriu, Richard J Auchus, Irina Bancos, Beverly M K Biller\",\"doi\":\"10.1210/jendso/bvaf027\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Although most cases of endogenous Cushing syndrome are caused by a pituitary adenoma (Cushing disease), approximately one-third of patients present with ectopic or adrenal causes. Surgery is the first-line treatment for most patients with Cushing syndrome; however, medical therapy is an important management option for those who are not eligible for, refuse, or do not respond to surgery. Clinical experience demonstrating that osilodrostat, an oral 11β-hydroxylase inhibitor, is effective and well tolerated comes predominantly from phase III trials in patients with Cushing disease. Nonetheless, reports of its use in patients with ectopic or adrenal Cushing syndrome are increasing. These data highlight the importance of selecting the most appropriate starting dose and titration frequency while monitoring for adverse events, including those related to hypocortisolism and prolongation of the QT interval, to optimize treatment outcomes. Here we use illustrative case studies to discuss practical considerations for the management of patients with ectopic or adrenal Cushing syndrome and review published data on the use of osilodrostat in these patients. The case studies show that to achieve the goal of reducing cortisol levels in all etiologies of Cushing syndrome, management should be individualized according to each patient's disease severity, comorbidities, performance status, and response to treatment. This approach to osilodrostat treatment maximizes the benefits of effective cortisol control, leads to improvements in comorbid conditions, and may ameliorate quality of life for patients across all types and severities of Cushing syndrome.</p>\",\"PeriodicalId\":17334,\"journal\":{\"name\":\"Journal of the Endocrine Society\",\"volume\":\"9 4\",\"pages\":\"bvaf027\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-02-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915091/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Endocrine Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1210/jendso/bvaf027\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/3 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvaf027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/3 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Osilodrostat Treatment for Adrenal and Ectopic Cushing Syndrome: Integration of Clinical Studies With Case Presentations.
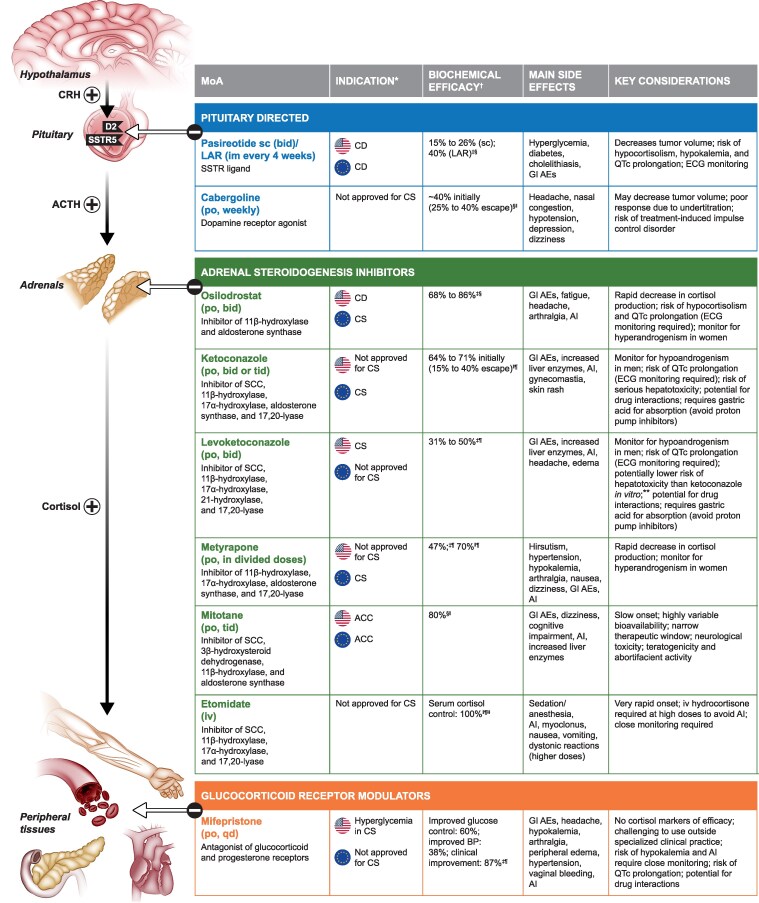
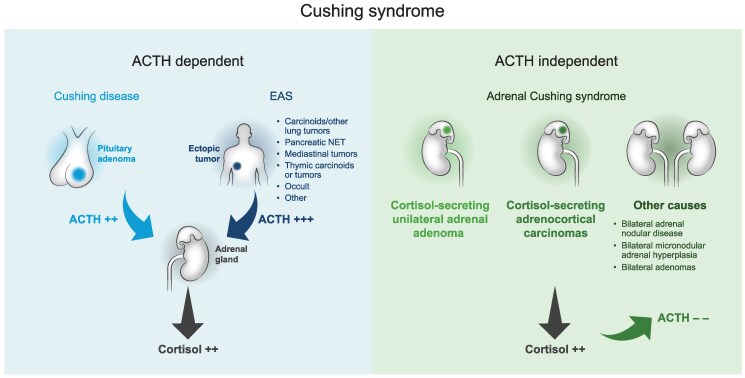
Although most cases of endogenous Cushing syndrome are caused by a pituitary adenoma (Cushing disease), approximately one-third of patients present with ectopic or adrenal causes. Surgery is the first-line treatment for most patients with Cushing syndrome; however, medical therapy is an important management option for those who are not eligible for, refuse, or do not respond to surgery. Clinical experience demonstrating that osilodrostat, an oral 11β-hydroxylase inhibitor, is effective and well tolerated comes predominantly from phase III trials in patients with Cushing disease. Nonetheless, reports of its use in patients with ectopic or adrenal Cushing syndrome are increasing. These data highlight the importance of selecting the most appropriate starting dose and titration frequency while monitoring for adverse events, including those related to hypocortisolism and prolongation of the QT interval, to optimize treatment outcomes. Here we use illustrative case studies to discuss practical considerations for the management of patients with ectopic or adrenal Cushing syndrome and review published data on the use of osilodrostat in these patients. The case studies show that to achieve the goal of reducing cortisol levels in all etiologies of Cushing syndrome, management should be individualized according to each patient's disease severity, comorbidities, performance status, and response to treatment. This approach to osilodrostat treatment maximizes the benefits of effective cortisol control, leads to improvements in comorbid conditions, and may ameliorate quality of life for patients across all types and severities of Cushing syndrome.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
