Marie Björkenstam, Emanuele Bobbio, Christian L Polte, Clara Hjalmarsson, Niklas Bergh, Elmir Omerovic, Entela Bollano
{"title":"急性心肌炎和不明原因急性胸痛的特点和预后:一项全国性的纵向队列研究。","authors":"Marie Björkenstam, Emanuele Bobbio, Christian L Polte, Clara Hjalmarsson, Niklas Bergh, Elmir Omerovic, Entela Bollano","doi":"10.1136/openhrt-2024-003050","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Acute myocarditis (AM) is a disease with variable prognosis, ranging from complete recovery to end-stage heart failure (HF) and death but often challenging to differentiate from unexplained acute chest pain (UCP) in the acute setting. This study examines the short-tem and long-term outcomes of AM compared with UCP, focusing on the risk of HF development.</p><p><strong>Methods: </strong>We used the Swedish Web System for Enhancement of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies-registry to identify patients >16 years admitted to hospital between 1 January 1998 and 31 December 2018 with either AM or UCP. Patients were followed for outcomes including mortality, rehospitalisation and HF development over both short-term (30 days) and long-term periods. Cox proportional hazards models were used to compare the risks, adjusting for demographic and clinical-related factors.</p><p><strong>Results: </strong>A total of 3792 patients with AM and 109 934 patients with UCP were included. Median follow-up time was 7.8 years (Q1, Q3; 3.4, 12.3). AM patients were younger compared with UCP patients, median age 37 years (Q1, Q3; 26, 52) vs 59 years (Q1, Q3; 49, 69) and more likely to be men (79.9% vs 51.4%, p<0.001). Comorbidity burden was less pronounced within the AM cohort. Chest pain was the most common presenting symptom in both groups. Mortality rate at 30 days (OR 3.75, 95% CI 1.9 to 7.3, p<0001) as well as long term (OR 2.0, 95% CI 1.69 to 2.39, p<0.001) were significantly higher in AM patients compared with UCP. AM patients were more likely to develop HF during follow-up (OR 2.3, 95% CI 1.81 to 2.93, p<0001).</p><p><strong>Conclusions: </strong>AM is associated with worse short-term and long-term outcomes compared with UCP, including a higher risk of developing HF even after the first year.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973765/pdf/","citationCount":"0","resultStr":"{\"title\":\"Characteristics and prognosis in acute myocarditis and unexplained acute chest pain: a nationwide longitudinal cohort study.\",\"authors\":\"Marie Björkenstam, Emanuele Bobbio, Christian L Polte, Clara Hjalmarsson, Niklas Bergh, Elmir Omerovic, Entela Bollano\",\"doi\":\"10.1136/openhrt-2024-003050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Acute myocarditis (AM) is a disease with variable prognosis, ranging from complete recovery to end-stage heart failure (HF) and death but often challenging to differentiate from unexplained acute chest pain (UCP) in the acute setting. This study examines the short-tem and long-term outcomes of AM compared with UCP, focusing on the risk of HF development.</p><p><strong>Methods: </strong>We used the Swedish Web System for Enhancement of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies-registry to identify patients >16 years admitted to hospital between 1 January 1998 and 31 December 2018 with either AM or UCP. Patients were followed for outcomes including mortality, rehospitalisation and HF development over both short-term (30 days) and long-term periods. Cox proportional hazards models were used to compare the risks, adjusting for demographic and clinical-related factors.</p><p><strong>Results: </strong>A total of 3792 patients with AM and 109 934 patients with UCP were included. Median follow-up time was 7.8 years (Q1, Q3; 3.4, 12.3). AM patients were younger compared with UCP patients, median age 37 years (Q1, Q3; 26, 52) vs 59 years (Q1, Q3; 49, 69) and more likely to be men (79.9% vs 51.4%, p<0.001). Comorbidity burden was less pronounced within the AM cohort. Chest pain was the most common presenting symptom in both groups. Mortality rate at 30 days (OR 3.75, 95% CI 1.9 to 7.3, p<0001) as well as long term (OR 2.0, 95% CI 1.69 to 2.39, p<0.001) were significantly higher in AM patients compared with UCP. AM patients were more likely to develop HF during follow-up (OR 2.3, 95% CI 1.81 to 2.93, p<0001).</p><p><strong>Conclusions: </strong>AM is associated with worse short-term and long-term outcomes compared with UCP, including a higher risk of developing HF even after the first year.</p>\",\"PeriodicalId\":19505,\"journal\":{\"name\":\"Open Heart\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-04-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973765/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/openhrt-2024-003050\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2024-003050","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
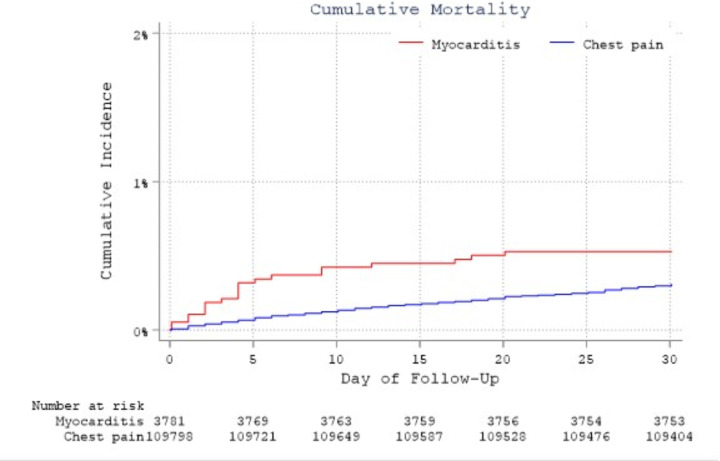
目的:急性心肌炎(AM)是一种预后多变的疾病,从完全恢复到终末期心力衰竭(HF)和死亡,但在急性情况下往往难以与不明原因的急性胸痛(UCP)区分。本研究比较了AM与UCP的短期和长期结果,重点关注HF发展的风险。方法:我们使用瑞典网络系统,根据推荐治疗方法评估心脏病的循证护理,以确定1998年1月1日至2018年12月31日期间住院的bb0 - 16岁AM或UCP患者。随访患者的结果包括短期(30天)和长期的死亡率、再住院率和心衰发展情况。Cox比例风险模型用于比较风险,调整了人口统计学和临床相关因素。结果:共纳入AM患者3792例,UCP患者109 934例。中位随访时间为7.8年(Q1, Q3;3.4, 12.3)。AM患者比UCP患者更年轻,中位年龄37岁(Q1, Q3;26,52) vs 59年(Q1, Q3;结论:与UCP相比,AM与较差的短期和长期预后相关,包括即使在第一年后发生HF的风险更高。
Characteristics and prognosis in acute myocarditis and unexplained acute chest pain: a nationwide longitudinal cohort study.
Aims: Acute myocarditis (AM) is a disease with variable prognosis, ranging from complete recovery to end-stage heart failure (HF) and death but often challenging to differentiate from unexplained acute chest pain (UCP) in the acute setting. This study examines the short-tem and long-term outcomes of AM compared with UCP, focusing on the risk of HF development.
Methods: We used the Swedish Web System for Enhancement of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies-registry to identify patients >16 years admitted to hospital between 1 January 1998 and 31 December 2018 with either AM or UCP. Patients were followed for outcomes including mortality, rehospitalisation and HF development over both short-term (30 days) and long-term periods. Cox proportional hazards models were used to compare the risks, adjusting for demographic and clinical-related factors.
Results: A total of 3792 patients with AM and 109 934 patients with UCP were included. Median follow-up time was 7.8 years (Q1, Q3; 3.4, 12.3). AM patients were younger compared with UCP patients, median age 37 years (Q1, Q3; 26, 52) vs 59 years (Q1, Q3; 49, 69) and more likely to be men (79.9% vs 51.4%, p<0.001). Comorbidity burden was less pronounced within the AM cohort. Chest pain was the most common presenting symptom in both groups. Mortality rate at 30 days (OR 3.75, 95% CI 1.9 to 7.3, p<0001) as well as long term (OR 2.0, 95% CI 1.69 to 2.39, p<0.001) were significantly higher in AM patients compared with UCP. AM patients were more likely to develop HF during follow-up (OR 2.3, 95% CI 1.81 to 2.93, p<0001).
Conclusions: AM is associated with worse short-term and long-term outcomes compared with UCP, including a higher risk of developing HF even after the first year.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
