{"title":"随机对照阿尔茨海默病抗炎预防试验(ADAPT)中的心脑血管事件","authors":"","doi":"10.1371/journal.pctr.0010033","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The Alzheimer's Disease Anti-inflammatory Prevention Trial (ADAPT) was designed to evaluate the conventional NSAID naproxen sodium and the selective COX-2 inhibitor celecoxib for primary prevention of Alzheimer's dementia (AD). On 17 December 2004, after the Adenoma Prevention with Celecoxib (APC) trial reported increased cardiovascular risks with celecoxib, the ADAPT Steering Committee suspended treatment and enrollment. This paper reports on cardiovascular and cerebrovascular events in ADAPT.</p><p><strong>Design: </strong>ADAPT is a randomized, placebo-controlled, parallel chemoprevention trial with 1-46 mo of follow-up.</p><p><strong>Setting: </strong>The trial was conducted at six field sites in the United States: Baltimore, Maryland; Boston, Massachusetts; Rochester, New York; Seattle, Washington; Sun City, Arizona; and Tampa, Florida.</p><p><strong>Participants: </strong>The 2,528 participants were aged 70 y and older with a family history of AD.</p><p><strong>Interventions: </strong>Study treatments were celecoxib (200 mg b.i.d.), naproxen sodium (220 mg b.i.d.), and placebo.</p><p><strong>Outcome measures: </strong>Outcome measures were deaths, along with nonfatal myocardial infarction (MI), stroke, congestive heart failure (CHF), transient ischemic attack (TIA), and antihypertensive treatment recorded from structured interviews at scheduled intervals. Cox proportional hazards regression was used to analyze these events individually and in several composites.</p><p><strong>Results: </strong>Counts (with 3-y incidence) of participants who experienced cardiovascular or cerebrovascular death, MI, stroke, CHF, or TIA in the celecoxib-, naproxen-, and placebo-treated groups were 28/717 (5.54%), 40/713 (8.25%), and 37/1070 (5.68%), respectively. This yielded a hazard ratio (95% confidence interval [CI]) for celecoxib of 1.10 (0.67-1.79) and for naproxen of 1.63 (1.04-2.55). Antihypertensive treatment was initiated in 160/440 (47.43%), 147/427 (45.00%), and 164/644 (34.08%). This yielded hazard ratios (CIs) of 1.56 for celecoxib (1.26-1.94) and 1.40 for naproxen (1.12-1.75).</p><p><strong>Conclusions: </strong>For celecoxib, ADAPT data do not show the same level of risk as those of the APC trial. The data for naproxen, although not definitive, are suggestive of increased cardiovascular and cerebrovascular risk.</p>","PeriodicalId":87416,"journal":{"name":"PLoS clinical trials","volume":"1 7","pages":"e33"},"PeriodicalIF":0.0000,"publicationDate":"2006-11-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1371/journal.pctr.0010033","citationCount":"3","resultStr":"{\"title\":\"Cardiovascular and cerebrovascular events in the randomized, controlled Alzheimer's Disease Anti-Inflammatory Prevention Trial (ADAPT).\",\"authors\":\"\",\"doi\":\"10.1371/journal.pctr.0010033\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The Alzheimer's Disease Anti-inflammatory Prevention Trial (ADAPT) was designed to evaluate the conventional NSAID naproxen sodium and the selective COX-2 inhibitor celecoxib for primary prevention of Alzheimer's dementia (AD). On 17 December 2004, after the Adenoma Prevention with Celecoxib (APC) trial reported increased cardiovascular risks with celecoxib, the ADAPT Steering Committee suspended treatment and enrollment. This paper reports on cardiovascular and cerebrovascular events in ADAPT.</p><p><strong>Design: </strong>ADAPT is a randomized, placebo-controlled, parallel chemoprevention trial with 1-46 mo of follow-up.</p><p><strong>Setting: </strong>The trial was conducted at six field sites in the United States: Baltimore, Maryland; Boston, Massachusetts; Rochester, New York; Seattle, Washington; Sun City, Arizona; and Tampa, Florida.</p><p><strong>Participants: </strong>The 2,528 participants were aged 70 y and older with a family history of AD.</p><p><strong>Interventions: </strong>Study treatments were celecoxib (200 mg b.i.d.), naproxen sodium (220 mg b.i.d.), and placebo.</p><p><strong>Outcome measures: </strong>Outcome measures were deaths, along with nonfatal myocardial infarction (MI), stroke, congestive heart failure (CHF), transient ischemic attack (TIA), and antihypertensive treatment recorded from structured interviews at scheduled intervals. Cox proportional hazards regression was used to analyze these events individually and in several composites.</p><p><strong>Results: </strong>Counts (with 3-y incidence) of participants who experienced cardiovascular or cerebrovascular death, MI, stroke, CHF, or TIA in the celecoxib-, naproxen-, and placebo-treated groups were 28/717 (5.54%), 40/713 (8.25%), and 37/1070 (5.68%), respectively. This yielded a hazard ratio (95% confidence interval [CI]) for celecoxib of 1.10 (0.67-1.79) and for naproxen of 1.63 (1.04-2.55). Antihypertensive treatment was initiated in 160/440 (47.43%), 147/427 (45.00%), and 164/644 (34.08%). This yielded hazard ratios (CIs) of 1.56 for celecoxib (1.26-1.94) and 1.40 for naproxen (1.12-1.75).</p><p><strong>Conclusions: </strong>For celecoxib, ADAPT data do not show the same level of risk as those of the APC trial. The data for naproxen, although not definitive, are suggestive of increased cardiovascular and cerebrovascular risk.</p>\",\"PeriodicalId\":87416,\"journal\":{\"name\":\"PLoS clinical trials\",\"volume\":\"1 7\",\"pages\":\"e33\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2006-11-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1371/journal.pctr.0010033\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS clinical trials\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pctr.0010033\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS clinical trials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pctr.0010033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Cardiovascular and cerebrovascular events in the randomized, controlled Alzheimer's Disease Anti-Inflammatory Prevention Trial (ADAPT).
Objectives: The Alzheimer's Disease Anti-inflammatory Prevention Trial (ADAPT) was designed to evaluate the conventional NSAID naproxen sodium and the selective COX-2 inhibitor celecoxib for primary prevention of Alzheimer's dementia (AD). On 17 December 2004, after the Adenoma Prevention with Celecoxib (APC) trial reported increased cardiovascular risks with celecoxib, the ADAPT Steering Committee suspended treatment and enrollment. This paper reports on cardiovascular and cerebrovascular events in ADAPT.
Design: ADAPT is a randomized, placebo-controlled, parallel chemoprevention trial with 1-46 mo of follow-up.
Setting: The trial was conducted at six field sites in the United States: Baltimore, Maryland; Boston, Massachusetts; Rochester, New York; Seattle, Washington; Sun City, Arizona; and Tampa, Florida.
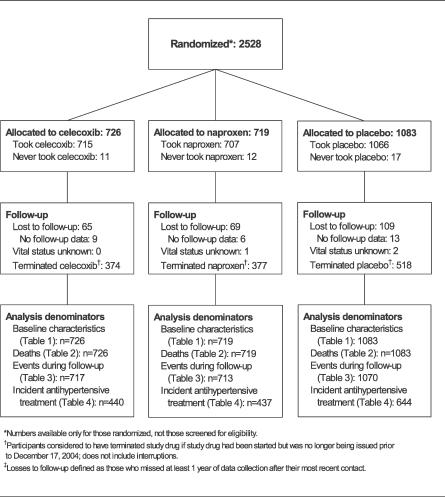
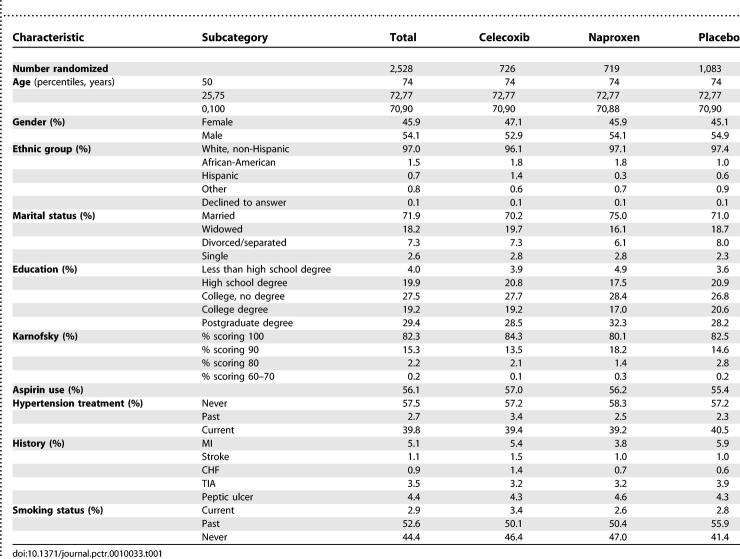
Participants: The 2,528 participants were aged 70 y and older with a family history of AD.
Interventions: Study treatments were celecoxib (200 mg b.i.d.), naproxen sodium (220 mg b.i.d.), and placebo.
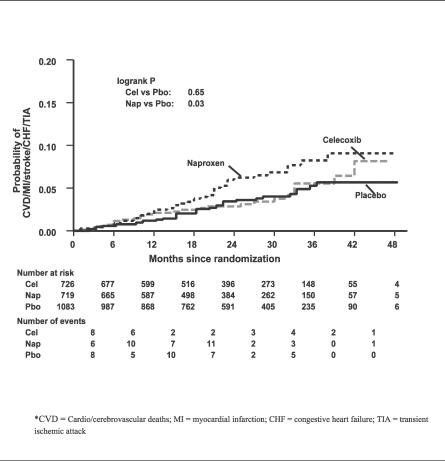
Outcome measures: Outcome measures were deaths, along with nonfatal myocardial infarction (MI), stroke, congestive heart failure (CHF), transient ischemic attack (TIA), and antihypertensive treatment recorded from structured interviews at scheduled intervals. Cox proportional hazards regression was used to analyze these events individually and in several composites.
Results: Counts (with 3-y incidence) of participants who experienced cardiovascular or cerebrovascular death, MI, stroke, CHF, or TIA in the celecoxib-, naproxen-, and placebo-treated groups were 28/717 (5.54%), 40/713 (8.25%), and 37/1070 (5.68%), respectively. This yielded a hazard ratio (95% confidence interval [CI]) for celecoxib of 1.10 (0.67-1.79) and for naproxen of 1.63 (1.04-2.55). Antihypertensive treatment was initiated in 160/440 (47.43%), 147/427 (45.00%), and 164/644 (34.08%). This yielded hazard ratios (CIs) of 1.56 for celecoxib (1.26-1.94) and 1.40 for naproxen (1.12-1.75).
Conclusions: For celecoxib, ADAPT data do not show the same level of risk as those of the APC trial. The data for naproxen, although not definitive, are suggestive of increased cardiovascular and cerebrovascular risk.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
