Eleanor Bailey, Nick Fenning, Sarah Chamberlain, Lindsey Devlin, James Hopkisson, Mathew Tomlinson
{"title":"男科实验室角*:使用协议限制的精子计数方法的验证","authors":"Eleanor Bailey, Nick Fenning, Sarah Chamberlain, Lindsey Devlin, James Hopkisson, Mathew Tomlinson","doi":"10.2164/jandrol.106.002188","DOIUrl":null,"url":null,"abstract":"<p>A variety of methods exist for counting sperm. Since the introduction of semen analysis, one of these methods, the hemocytometer, has been regarded as the gold standard by andrology laboratories and the World Health Organization (WHO, 1999). The flexible features of this approach, involving fixation and immobilization of sperm, dilution of highly concentrated samples, and the counting of sperm in a single plane, contribute to the accuracy of the Improved Neubauer hemocytometer and its relative ease of use. This method is strongly accepted within andrology clinics and has been clinically validated by a number of studies (Dunphy et al, 1989; Tomlinson et al, 1996, 1999; Guzick et al, 2001).</p><p>As technology and techniques improve, manufacturers are continually trying to develop newer, simpler, quicker and more accurate methods for determining sperm concentration. Busy assisted reproduction technology (ART) laboratories in particular would find a quicker yet comparatively accurate method highly desirable, since sperm counting is an essential part of the semen preparation process. Although modern methods may be faster, since unfixed, undiluted semen is used, some labs find these analyses more difficult to use and believe that the counting of motile sperm may produce erroneous results. Furthermore, the WHO states that the newly introduced methods “are convenient in that they can be used without dilution of the specimen, but that they may lack the accuracy of the hemocytometer technique especially for highly viscous and/or heterogeneous specimens. If such chambers are to be used, their adequate accuracy and precision must be established by comparison with hemocytometers” (WHO, 1999).</p><p>In addition, it is now a requirement of laboratory accreditation systems that laboratories provide clinical validation for all methods used (ie, demonstrate that they are “fit for purpose”). Currently, the only sperm counting method with a considerable body of evidence to support and clincally justify its use is the hemocytometer (Mortimer, 1994; WHO, 1999).</p><p>When using the hemocytometer, the sperm number is calculated using a fixed volume of semen under the coverslip and counting the sperm in a single plane. A significant association between pregnancy and the sperm concentration measured has consistently been shown for this method (Dunphy et al, 1989; Tomlinson et al, 1996, 1999; Guzick et al, 2001). Thus, 64% of laboratories involved in the analysis of semen use this method routinely (Keel et al, 2000).</p><p>However, despite its validity as a method, the use of hemocytometry is thought by many to be inconvenient, in that the hemocytometer must be cleaned and assembled prior to each counting event and it involves the use of dilution techniques that can introduce errors, either due to poor technique or the viscous nature of the semen itself. Mathematical mistakes can occur when applying the correction factor to determine the eventual counts, and the recommended dilution method uses fixatives, such as formal saline, which are often a reason for rejection of the method by embryologists in IVF laboratories.</p><p>Comparisons of other counting chambers with the hemocytometer, particularly those marketed as easy-to-use 1-step methods have generally not been favorable. Makler sperm counts have been shown to be generally higher than the corresponding counts obtained with the hemocytometer (Coetzee and Menkveld, 2001; Sukcharoen et al, 1994). Indeed, Ginsburg and Armant (1990) have found the Makler chamber counts to be 62% higher than those obtained with the hemocytometer when using latex beads. Other methods, such as the Leja slide (Gynotec Malden, Nieuw-Vennep, The Netherlands) or the Microcell (Conception Technologies, San Diego, Calif) have been shown to produce significantly lower average sperm counts as compared to the hemocytometer. In particular, marked differences were seen at high concentrations (Tomlinson et al, 2001). A number of potential sources of error have been suggested to cause these discrepancies when using 1-step methods. First, the recommendation that motile sperm are counted, which may mean a single spermatozoon is counted more than once or not counted at all. Second and perhaps more significantly is the phenomenum that affects capillary-loaded chambers, such as the Leja and Microcell slides, which is known as the Segre-Silberberg (SS) effect (Segre and Silberberg, 1961). The SS effect results in high-gradient fluid flow in thin capillary-loaded slides, which results in the sperm suspension being forced transversely towards the walls, causing uneven cell dispersion throughout the chamber. New measures have recently been introduced to compensate for this phenomenon. A correction factor is used, which makes allowances for changes in sample viscosity and appears to improve the performance of there slides in terms of agreement with the hemocytometer (Douglas-Hamilton et al, 2005). Third, many of the studies that have compared the performances of various methods with the gold standard of the hemocytometer are problematic in terms of the choice of statistics. Unfortunately, many of these studies have focused on analysing differences across a range of sperm counts, whereas a proper and more detailed analysis is one that compares each and every individual count and measures the agreement between these 2 parameters. Therefore, in the present study, we employ limits of agreement (LoA) to analyse comparative data. This approach, which is based on graphical techniques and simple calculations, allows comparisons between new measurement techniques (ie, the Leja and Makler chambers) and an established method (ie, the hemocytometer). Thus, we can evaluate whether the methods agree sufficiently for the new method to replace the old method and we can decide if the differences between the 2 methods are sufficiently small for the methods to be used interchangeably (Bland and Altman, 1986).</p><p>The objectives of the present study were: 1) to determine whether the sperm counts obtained using the Leja slide and Makler chamber compare favorably with the counts obtained using the hemocytometer; 2) to determine whether the accuracy and reliability of sperm counts obtained using the Leja slide and the Makler chamber are improved by prior fixation and dilution of the specimen; 3) to determine whether the sperm counts obtained using the Leja slide compared more favorably with the counts obtained using the hemocytometer when correction is made for the SS effect; and 4) to determine by the use of LOA whether these methods can be considered to be interchangeable, thereby providing validation for their routine clinical application.</p><p>The aim of the present investigation was to determine whether three different methods used for analyzing sperm counts in a fertility laboratory setting could be considered to be interchangable. All 3 methods are currently in use in laboratories throughout the United Kingdom and worlwide.</p><p>The ICC, CV, and CI values show that all the counting methods have a particularly high degree of repeatability/reliability. The hemocytometer was the most reliable method, with the highest ICC, lowest CV, and smallest 95% CI. This finding partially supports the hemocytometer as the gold standard method, although its precision is clearly not high. The Leja was the next most reliable method, although it was more reliable without the fixation/dilution step, which suggests that this step may introduce a degree of error. The analyses showed the Makler chamber to have significantly poorer reliability than the hemocytometer or Leja. The ICC of the Makler chamber was much lower for both undiluted and diluted samples, and the CV and CI showed great variability between the repeated counts.</p><p>The LOA analysis showed that the Leja slide could be compared favourably with the hemocytometer, particularly for the 1:1 dilutions. However, despite showing that the Leja 1:1 and hemocytometer have a mean difference of zero, the standard deviation was calculated as 0.9. Thus, the LOA lie between −2.04 and 1.7, which means that in a worst case scenario, specimens that contain 5 × 10<sup>6</sup>/mL in the hemocytometer could have counts between zero and 16 × 10<sup>6</sup> sperm/mL. Similarly, the Leja method could determine the concentration of a sample with 20 × 10<sup>6</sup> sperm/mL to be between 6 × 10<sup>6</sup> and 38 × 10<sup>6</sup> sperm/mL. Although the latter form of analysis may at first glance appear to lack precision, the same principle can be applied to repeat counts using the same chamber. In other words, in most cases, the difference between the chambers is no worse than repeated measures using the same chamber. There will always be occasional outliers and perhaps more outliers when semen is the test fluid in question and this could be due to any one of a number of factors (eg, hyperviscosity, sampling error, mathematical error, diluting error or chamber flaws). When assessing the agreement and interchangeability of a method, it has to be put in the context of the level of expectation. As there is innate variability in hemocytometer counts using either repeated measures or between individuals, we will undoubtedly detect differences when comparing this with other chambers. In this context, the Leja slide could be viewed as being interchangeable with the hemocytometer, particularly if the sample is first fixed and diluted.</p><p>All of the results show very clearly that applying the SS factor increases the level of agreement between the Leja counts and hemocytometer counts, as expected. This improvement was more pronounced for the 1:1 diluted samples, for which the mean difference with the hemocytometer became 0 for the modified Leja counts. This is reassuring, since the Leja Instruction Manual states that the correction factors were initially calculated by calibrating the Leja with the Improved Neubauer chamber.</p><p>The Makler chamber showed extremely poor agreement with all the other methods and had a tendency to overestimate sperm counts. In the worst case, a sample of 20 × 10<sup>6</sup>/mL could be found have between 9.2 × 10<sup>6</sup> and 58.9 × 10<sup>6</sup> sperm/mL, which could have serious consequences for the diagnostic or treatment laboratory. This finding supports previous studies that have found that the Makler produces high sperm counts (Ginsburg and Armant, 1990; Sukcharoen et al, 1994; Seaman et al, 1996; Coetzee and Menkveld, 2001; Lu et al, 2004). Laboratories provided with a latex bead solution with a known, fixed concentration of 35 × 10<sup>6</sup> sperm/mL determined the concentration on the Makler to be 53.5 × 10<sup>6</sup>/mL on average. A similar study conducted by Seaman et al (1996) found that the Makler chamber overestimated the known bead concentrations by as much as 50%.</p><p>The counts determined using the Leja slide were significantly different from the counts obtained using the hemocytometer (<i>P</i> < .05), unless they specimens were first fixed and diluted. The Leja median was significantly lower than that of the hemocytometer, and this finding was supported by the LOA analysis, which showed that the Leja on average underestimated the sperm count when undiluted semen was used. This underestimation was consistent throughout the data distribution and was not related to the sperm concentrations of the samples. It was expected that the Leja would underestimate the sperm count when compared to the hemocytometer, since a study by Tomlinson et al (2001) has found Leja counts to be significantly lower (<i>P</i> < .0001) than the corresponding hemocytometer readings, although these counts were performed using a previous version of the Leja chamber and without knowledge of the SS factor.</p><p>Fixing and diluting the samples for analysis by the Makler method reduced the mean difference and increased the level of agreement with the hemocytometer counts. However the counts produced in the Makler chamber were significantly higher than those in the hemocytometer, regardless of whether they were performed on undiluted or diluted specimens.</p><p>In some instances, laboratories are clearly willing to compromise on the accuracy of sperm parameter measurements in order to maximise speed and convenience. The preference for methods of sperm counting and the selection of counting chambers may in many cases reflect the type of clinical service and the level of expertise provided by a particular laboratory. It is known that many IVF labs favor the 1-step methods owing to their convenience, even though this could indirectly compromise practice, in that future treatment decisions based on sperm thresholds could be derived from erroneous data.</p><p>It has been suggested previously that using different methodologies to analyze sperm concentrations is the major cause of variation in sperm counts between laboratories (Auger et al, 2000). Owing to disagreements between laboratories, a patient could be classified as normal by one and as infertile by another (Neuwinger et al, 1990). This has been known for some time and is supported by the findings of the present study. Sperm concentration discrepancies between the Leja and hemocytometer affected the diagnosis of 21 patients in the present study. Such erroneous diagnoses could have serious consequences for patients, some of whom may be misidentified as infertile (according to the WHO criteria), which could in turn have negative psychosocial implications and mean that some individuals would not receive the appropriate assistance in achieving pregnancy.</p><p>We know from previous studies that many of the current methods in use carry a degree of error, which is high in comparison with many other types of diagnostic testing, many of which are fully automated. Simple factors, such as the inherent viscosity and heterogeneity of semen, incomplete mixing, errors in pipetting, mathematics, and transcribing, are all contributory. It is likely that the general lack of consensus and lack of strong evidence linking sperm concentration with either natural or assisted conception are due to either poor practice or the intrinsic inaccuracies of many of the methods used.</p><p>Another source of error, and possibly the most significant, is sampling error. By its very nature, 1 small microlitre aliquot of semen may have very different qualities when compared to another. Therefore, only by better mixing, increasing the volume of seminal fluid, and increasing the number of sperm counted per analysis can we hope to improve the current degrees of accuracy and precision. However, this has to balanced against whether there is a need for such a degree of accuracy and also whether it is a good use of resources.</p><p>The relatively high risk of error during the analysis, be it due to the method used, sampling error, transcription or a case of mistaken identity, raises the question as to whether a diagnosis should ever be based upon the findings of a single semen sample. Adding in other variables, such as whether the sample is complete, length of sexual abstinence, illness, stress, and medications, all of which are known to affect sperm count, ensures that the relationship between male fertility and sperm count is weaker than perhaps it should be. The unfortunate consequence of this is that semen analysis continues to demonstrate poor predictive value in terms of either natural or assisted conception (eg, IUI, IVF, and ICSI).</p><p>The hemocytometer method has long been the accepted standard for the assessment of sperm concentration. Indeed, the WHO recommends in its guide to semen analysis (1999) that a hemocytometer, such as the Improved Neubauer, should be used for sperm concentration measurements. Despite this, an estimated 64% of laboratories used the hemocytometer, while 26% used the Makler chamber, and the remainder used alternative disposable methods, such as the Leja slide (Keel et al, 2000). One-step disposable methods, such as the Leja slide, and re-usable glass chambers, such as the Makler, have been put forward as convenient alternatives. The present study suggests that there is limited agreement between all of these methods, with the widest discrepancy between hemocytometry and the Makler method.</p><p>If the standard Leja method was modified by fixing and diluting the sample, the overall agreement with hemocytometery was very good. Therefore, if it can be shown that the 2 methods are likely to give the same counts, the 2 methods could be said to be interchangble, providing a degree of validation for the Leja method. The hemocytometer is marginally better in terms of precison but, like all of the methods, has intrinsic weaknesses in terms of reliability and repeatability, which may be related to the test fluid in question.</p><p>In conclusion, there is little to choose between the hemocytometer and diluted Leja method in terms of average sperm count, which suggests that the Leja slide may be suitable for use in clinical pactice. In contrast, the Makler method showed very poor agreement throughout the entire data range and cannot be recommended. The limited agreement seen between all 3 methods and their apparent lack of precision is a cause for concern. If the WHO continues to recommend the hemocytometer as the gold standard method, then there should at least be a reappraisal of the method. Testing inaccuracies are often blamed on poor technique or technical training, yet it is clear that all methods for sperm counting have inherent weaknesses. Laboratories must be better equipped in order to provide users of their service (eg, Ob/Gyn clinicians). with proper information about the test, including its limitations and the expected level of accuracy and precision, in order to allow efficient management of their male patients.</p>","PeriodicalId":15029,"journal":{"name":"Journal of andrology","volume":"28 3","pages":"364-373"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2164/jandrol.106.002188","citationCount":"42","resultStr":"{\"title\":\"ANDROLOGY LAB CORNER*: Validation of Sperm Counting Methods Using Limits of Agreement\",\"authors\":\"Eleanor Bailey, Nick Fenning, Sarah Chamberlain, Lindsey Devlin, James Hopkisson, Mathew Tomlinson\",\"doi\":\"10.2164/jandrol.106.002188\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A variety of methods exist for counting sperm. Since the introduction of semen analysis, one of these methods, the hemocytometer, has been regarded as the gold standard by andrology laboratories and the World Health Organization (WHO, 1999). The flexible features of this approach, involving fixation and immobilization of sperm, dilution of highly concentrated samples, and the counting of sperm in a single plane, contribute to the accuracy of the Improved Neubauer hemocytometer and its relative ease of use. This method is strongly accepted within andrology clinics and has been clinically validated by a number of studies (Dunphy et al, 1989; Tomlinson et al, 1996, 1999; Guzick et al, 2001).</p><p>As technology and techniques improve, manufacturers are continually trying to develop newer, simpler, quicker and more accurate methods for determining sperm concentration. Busy assisted reproduction technology (ART) laboratories in particular would find a quicker yet comparatively accurate method highly desirable, since sperm counting is an essential part of the semen preparation process. Although modern methods may be faster, since unfixed, undiluted semen is used, some labs find these analyses more difficult to use and believe that the counting of motile sperm may produce erroneous results. Furthermore, the WHO states that the newly introduced methods “are convenient in that they can be used without dilution of the specimen, but that they may lack the accuracy of the hemocytometer technique especially for highly viscous and/or heterogeneous specimens. If such chambers are to be used, their adequate accuracy and precision must be established by comparison with hemocytometers” (WHO, 1999).</p><p>In addition, it is now a requirement of laboratory accreditation systems that laboratories provide clinical validation for all methods used (ie, demonstrate that they are “fit for purpose”). Currently, the only sperm counting method with a considerable body of evidence to support and clincally justify its use is the hemocytometer (Mortimer, 1994; WHO, 1999).</p><p>When using the hemocytometer, the sperm number is calculated using a fixed volume of semen under the coverslip and counting the sperm in a single plane. A significant association between pregnancy and the sperm concentration measured has consistently been shown for this method (Dunphy et al, 1989; Tomlinson et al, 1996, 1999; Guzick et al, 2001). Thus, 64% of laboratories involved in the analysis of semen use this method routinely (Keel et al, 2000).</p><p>However, despite its validity as a method, the use of hemocytometry is thought by many to be inconvenient, in that the hemocytometer must be cleaned and assembled prior to each counting event and it involves the use of dilution techniques that can introduce errors, either due to poor technique or the viscous nature of the semen itself. Mathematical mistakes can occur when applying the correction factor to determine the eventual counts, and the recommended dilution method uses fixatives, such as formal saline, which are often a reason for rejection of the method by embryologists in IVF laboratories.</p><p>Comparisons of other counting chambers with the hemocytometer, particularly those marketed as easy-to-use 1-step methods have generally not been favorable. Makler sperm counts have been shown to be generally higher than the corresponding counts obtained with the hemocytometer (Coetzee and Menkveld, 2001; Sukcharoen et al, 1994). Indeed, Ginsburg and Armant (1990) have found the Makler chamber counts to be 62% higher than those obtained with the hemocytometer when using latex beads. Other methods, such as the Leja slide (Gynotec Malden, Nieuw-Vennep, The Netherlands) or the Microcell (Conception Technologies, San Diego, Calif) have been shown to produce significantly lower average sperm counts as compared to the hemocytometer. In particular, marked differences were seen at high concentrations (Tomlinson et al, 2001). A number of potential sources of error have been suggested to cause these discrepancies when using 1-step methods. First, the recommendation that motile sperm are counted, which may mean a single spermatozoon is counted more than once or not counted at all. Second and perhaps more significantly is the phenomenum that affects capillary-loaded chambers, such as the Leja and Microcell slides, which is known as the Segre-Silberberg (SS) effect (Segre and Silberberg, 1961). The SS effect results in high-gradient fluid flow in thin capillary-loaded slides, which results in the sperm suspension being forced transversely towards the walls, causing uneven cell dispersion throughout the chamber. New measures have recently been introduced to compensate for this phenomenon. A correction factor is used, which makes allowances for changes in sample viscosity and appears to improve the performance of there slides in terms of agreement with the hemocytometer (Douglas-Hamilton et al, 2005). Third, many of the studies that have compared the performances of various methods with the gold standard of the hemocytometer are problematic in terms of the choice of statistics. Unfortunately, many of these studies have focused on analysing differences across a range of sperm counts, whereas a proper and more detailed analysis is one that compares each and every individual count and measures the agreement between these 2 parameters. Therefore, in the present study, we employ limits of agreement (LoA) to analyse comparative data. This approach, which is based on graphical techniques and simple calculations, allows comparisons between new measurement techniques (ie, the Leja and Makler chambers) and an established method (ie, the hemocytometer). Thus, we can evaluate whether the methods agree sufficiently for the new method to replace the old method and we can decide if the differences between the 2 methods are sufficiently small for the methods to be used interchangeably (Bland and Altman, 1986).</p><p>The objectives of the present study were: 1) to determine whether the sperm counts obtained using the Leja slide and Makler chamber compare favorably with the counts obtained using the hemocytometer; 2) to determine whether the accuracy and reliability of sperm counts obtained using the Leja slide and the Makler chamber are improved by prior fixation and dilution of the specimen; 3) to determine whether the sperm counts obtained using the Leja slide compared more favorably with the counts obtained using the hemocytometer when correction is made for the SS effect; and 4) to determine by the use of LOA whether these methods can be considered to be interchangeable, thereby providing validation for their routine clinical application.</p><p>The aim of the present investigation was to determine whether three different methods used for analyzing sperm counts in a fertility laboratory setting could be considered to be interchangable. All 3 methods are currently in use in laboratories throughout the United Kingdom and worlwide.</p><p>The ICC, CV, and CI values show that all the counting methods have a particularly high degree of repeatability/reliability. The hemocytometer was the most reliable method, with the highest ICC, lowest CV, and smallest 95% CI. This finding partially supports the hemocytometer as the gold standard method, although its precision is clearly not high. The Leja was the next most reliable method, although it was more reliable without the fixation/dilution step, which suggests that this step may introduce a degree of error. The analyses showed the Makler chamber to have significantly poorer reliability than the hemocytometer or Leja. The ICC of the Makler chamber was much lower for both undiluted and diluted samples, and the CV and CI showed great variability between the repeated counts.</p><p>The LOA analysis showed that the Leja slide could be compared favourably with the hemocytometer, particularly for the 1:1 dilutions. However, despite showing that the Leja 1:1 and hemocytometer have a mean difference of zero, the standard deviation was calculated as 0.9. Thus, the LOA lie between −2.04 and 1.7, which means that in a worst case scenario, specimens that contain 5 × 10<sup>6</sup>/mL in the hemocytometer could have counts between zero and 16 × 10<sup>6</sup> sperm/mL. Similarly, the Leja method could determine the concentration of a sample with 20 × 10<sup>6</sup> sperm/mL to be between 6 × 10<sup>6</sup> and 38 × 10<sup>6</sup> sperm/mL. Although the latter form of analysis may at first glance appear to lack precision, the same principle can be applied to repeat counts using the same chamber. In other words, in most cases, the difference between the chambers is no worse than repeated measures using the same chamber. There will always be occasional outliers and perhaps more outliers when semen is the test fluid in question and this could be due to any one of a number of factors (eg, hyperviscosity, sampling error, mathematical error, diluting error or chamber flaws). When assessing the agreement and interchangeability of a method, it has to be put in the context of the level of expectation. As there is innate variability in hemocytometer counts using either repeated measures or between individuals, we will undoubtedly detect differences when comparing this with other chambers. In this context, the Leja slide could be viewed as being interchangeable with the hemocytometer, particularly if the sample is first fixed and diluted.</p><p>All of the results show very clearly that applying the SS factor increases the level of agreement between the Leja counts and hemocytometer counts, as expected. This improvement was more pronounced for the 1:1 diluted samples, for which the mean difference with the hemocytometer became 0 for the modified Leja counts. This is reassuring, since the Leja Instruction Manual states that the correction factors were initially calculated by calibrating the Leja with the Improved Neubauer chamber.</p><p>The Makler chamber showed extremely poor agreement with all the other methods and had a tendency to overestimate sperm counts. In the worst case, a sample of 20 × 10<sup>6</sup>/mL could be found have between 9.2 × 10<sup>6</sup> and 58.9 × 10<sup>6</sup> sperm/mL, which could have serious consequences for the diagnostic or treatment laboratory. This finding supports previous studies that have found that the Makler produces high sperm counts (Ginsburg and Armant, 1990; Sukcharoen et al, 1994; Seaman et al, 1996; Coetzee and Menkveld, 2001; Lu et al, 2004). Laboratories provided with a latex bead solution with a known, fixed concentration of 35 × 10<sup>6</sup> sperm/mL determined the concentration on the Makler to be 53.5 × 10<sup>6</sup>/mL on average. A similar study conducted by Seaman et al (1996) found that the Makler chamber overestimated the known bead concentrations by as much as 50%.</p><p>The counts determined using the Leja slide were significantly different from the counts obtained using the hemocytometer (<i>P</i> < .05), unless they specimens were first fixed and diluted. The Leja median was significantly lower than that of the hemocytometer, and this finding was supported by the LOA analysis, which showed that the Leja on average underestimated the sperm count when undiluted semen was used. This underestimation was consistent throughout the data distribution and was not related to the sperm concentrations of the samples. It was expected that the Leja would underestimate the sperm count when compared to the hemocytometer, since a study by Tomlinson et al (2001) has found Leja counts to be significantly lower (<i>P</i> < .0001) than the corresponding hemocytometer readings, although these counts were performed using a previous version of the Leja chamber and without knowledge of the SS factor.</p><p>Fixing and diluting the samples for analysis by the Makler method reduced the mean difference and increased the level of agreement with the hemocytometer counts. However the counts produced in the Makler chamber were significantly higher than those in the hemocytometer, regardless of whether they were performed on undiluted or diluted specimens.</p><p>In some instances, laboratories are clearly willing to compromise on the accuracy of sperm parameter measurements in order to maximise speed and convenience. The preference for methods of sperm counting and the selection of counting chambers may in many cases reflect the type of clinical service and the level of expertise provided by a particular laboratory. It is known that many IVF labs favor the 1-step methods owing to their convenience, even though this could indirectly compromise practice, in that future treatment decisions based on sperm thresholds could be derived from erroneous data.</p><p>It has been suggested previously that using different methodologies to analyze sperm concentrations is the major cause of variation in sperm counts between laboratories (Auger et al, 2000). Owing to disagreements between laboratories, a patient could be classified as normal by one and as infertile by another (Neuwinger et al, 1990). This has been known for some time and is supported by the findings of the present study. Sperm concentration discrepancies between the Leja and hemocytometer affected the diagnosis of 21 patients in the present study. Such erroneous diagnoses could have serious consequences for patients, some of whom may be misidentified as infertile (according to the WHO criteria), which could in turn have negative psychosocial implications and mean that some individuals would not receive the appropriate assistance in achieving pregnancy.</p><p>We know from previous studies that many of the current methods in use carry a degree of error, which is high in comparison with many other types of diagnostic testing, many of which are fully automated. Simple factors, such as the inherent viscosity and heterogeneity of semen, incomplete mixing, errors in pipetting, mathematics, and transcribing, are all contributory. It is likely that the general lack of consensus and lack of strong evidence linking sperm concentration with either natural or assisted conception are due to either poor practice or the intrinsic inaccuracies of many of the methods used.</p><p>Another source of error, and possibly the most significant, is sampling error. By its very nature, 1 small microlitre aliquot of semen may have very different qualities when compared to another. Therefore, only by better mixing, increasing the volume of seminal fluid, and increasing the number of sperm counted per analysis can we hope to improve the current degrees of accuracy and precision. However, this has to balanced against whether there is a need for such a degree of accuracy and also whether it is a good use of resources.</p><p>The relatively high risk of error during the analysis, be it due to the method used, sampling error, transcription or a case of mistaken identity, raises the question as to whether a diagnosis should ever be based upon the findings of a single semen sample. Adding in other variables, such as whether the sample is complete, length of sexual abstinence, illness, stress, and medications, all of which are known to affect sperm count, ensures that the relationship between male fertility and sperm count is weaker than perhaps it should be. The unfortunate consequence of this is that semen analysis continues to demonstrate poor predictive value in terms of either natural or assisted conception (eg, IUI, IVF, and ICSI).</p><p>The hemocytometer method has long been the accepted standard for the assessment of sperm concentration. Indeed, the WHO recommends in its guide to semen analysis (1999) that a hemocytometer, such as the Improved Neubauer, should be used for sperm concentration measurements. Despite this, an estimated 64% of laboratories used the hemocytometer, while 26% used the Makler chamber, and the remainder used alternative disposable methods, such as the Leja slide (Keel et al, 2000). One-step disposable methods, such as the Leja slide, and re-usable glass chambers, such as the Makler, have been put forward as convenient alternatives. The present study suggests that there is limited agreement between all of these methods, with the widest discrepancy between hemocytometry and the Makler method.</p><p>If the standard Leja method was modified by fixing and diluting the sample, the overall agreement with hemocytometery was very good. Therefore, if it can be shown that the 2 methods are likely to give the same counts, the 2 methods could be said to be interchangble, providing a degree of validation for the Leja method. The hemocytometer is marginally better in terms of precison but, like all of the methods, has intrinsic weaknesses in terms of reliability and repeatability, which may be related to the test fluid in question.</p><p>In conclusion, there is little to choose between the hemocytometer and diluted Leja method in terms of average sperm count, which suggests that the Leja slide may be suitable for use in clinical pactice. In contrast, the Makler method showed very poor agreement throughout the entire data range and cannot be recommended. The limited agreement seen between all 3 methods and their apparent lack of precision is a cause for concern. If the WHO continues to recommend the hemocytometer as the gold standard method, then there should at least be a reappraisal of the method. Testing inaccuracies are often blamed on poor technique or technical training, yet it is clear that all methods for sperm counting have inherent weaknesses. Laboratories must be better equipped in order to provide users of their service (eg, Ob/Gyn clinicians). with proper information about the test, including its limitations and the expected level of accuracy and precision, in order to allow efficient management of their male patients.</p>\",\"PeriodicalId\":15029,\"journal\":{\"name\":\"Journal of andrology\",\"volume\":\"28 3\",\"pages\":\"364-373\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-01-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.2164/jandrol.106.002188\",\"citationCount\":\"42\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of andrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.2164/jandrol.106.002188\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of andrology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.2164/jandrol.106.002188","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 42
摘要
精子计数的方法多种多样。自从采用精液分析以来,其中一种方法,血细胞计,已被男科实验室和世界卫生组织视为金标准(卫生组织,1999年)。这种方法的灵活特点,包括固定和固定精子,稀释高浓度的样本,以及在一个平面上计数精子,有助于改进Neubauer血细胞计的准确性和相对易于使用。这种方法在男科诊所被广泛接受,并得到了许多研究的临床验证(Dunphy et al, 1989;Tomlinson等人,1996,1999;Guzick et al, 2001)。随着技术和工艺的进步,制造商不断尝试开发更新、更简单、更快速和更准确的方法来测定精子浓度。忙碌的辅助生殖技术(ART)实验室尤其会发现一种更快但相对准确的方法是非常可取的,因为精子计数是精液制备过程的重要组成部分。尽管现代方法可能更快,但由于使用的是未固定的、未稀释的精液,一些实验室发现这些分析更难以使用,并认为对活动精子的计数可能会产生错误的结果。此外,世界卫生组织指出,新引入的方法“方便,因为它们可以在不稀释标本的情况下使用,但它们可能缺乏血细胞计技术的准确性,特别是对于高粘性和/或异质性标本。”如果要使用这种腔室,必须通过与血细胞计的比较来确定其足够的准确性和精密度”(WHO, 1999)。此外,实验室认可系统现在要求实验室为所使用的所有方法提供临床验证(即证明它们“适合目的”)。目前,唯一有大量证据支持和临床证明其使用的精子计数方法是血细胞计(Mortimer, 1994;世卫组织,1999年)。当使用血细胞计时,精子数量是通过盖盖下固定体积的精液来计算的,并将精子计数在一个平面上。怀孕和精子浓度测量之间的显著关联一直被这种方法所证实(Dunphy et al ., 1989;Tomlinson等人,1996,1999;Guzick et al, 2001)。因此,参与精液分析的实验室中有64%经常使用这种方法(Keel et al, 2000)。然而,尽管它作为一种方法是有效的,但许多人认为使用血细胞计是不方便的,因为血细胞计必须在每次计数事件之前进行清洁和组装,并且它涉及使用稀释技术,这可能会由于技术差或精液本身的粘性而引入错误。当使用校正因子来确定最终计数时,可能会出现数学错误,并且推荐的稀释方法使用固定剂,如生理盐水,这通常是试管婴儿实验室胚胎学家拒绝使用该方法的原因。其他计数室与血细胞计的比较,特别是那些市场上易于使用的一步法,通常是不利的。Makler精子计数已被证明通常高于血细胞计获得的相应计数(Coetzee和Menkveld, 2001;Sukcharoen et al ., 1994)。事实上,Ginsburg和Armant(1990)发现,使用乳胶珠时,马克勒室计数比使用血细胞计获得的计数高62%。其他方法,如Leja玻片(Gynotec Malden, Nieuw-Vennep,荷兰)或Microcell (Conception Technologies, San Diego, california)已被证明比血细胞计产生的平均精子数量要低得多。特别是在高浓度时,可以看到明显的差异(Tomlinson等人,2001年)。在使用一步法时,有许多潜在的错误来源会导致这些差异。首先,建议对活动精子进行计数,这可能意味着对单个精子进行多次计数或根本不进行计数。其次,也许更重要的是影响毛细血管负载腔的现象,如Leja和Microcell载玻片,这被称为Segre-Silberberg (SS)效应(Segre和Silberberg, 1961)。SS效应导致高梯度流体在薄的毛细血管载玻片中流动,这导致精子悬浮液被迫横向向细胞壁移动,导致细胞在整个腔室中的分散不均匀。最近采取了新的措施来弥补这一现象。校正因子的使用,允许样品粘度的变化,似乎提高了玻片的性能,与血细胞计的一致性(Douglas-Hamilton et al, 2005)。 第三,许多将各种方法的性能与血细胞计的金标准进行比较的研究在统计数据的选择方面存在问题。不幸的是,许多这样的研究都集中在分析精子数量的差异上,而一个适当的、更详细的分析是比较每一个个体的数量,并衡量这两个参数之间的一致性。因此,在本研究中,我们采用协议限制(LoA)来分析比较数据。这种方法基于图形技术和简单的计算,可以比较新的测量技术(如Leja和Makler腔)和已建立的方法(如血细胞计)。因此,我们可以评估方法是否足够一致,以新方法取代旧方法,我们可以决定两种方法之间的差异是否足够小,可以互换使用(Bland和Altman, 1986)。本研究的目的是:1)确定使用Leja载玻片和Makler腔获得的精子数量是否与使用血细胞计获得的精子数量相比较;2)通过事先固定和稀释标本,确定Leja载玻片和Makler室获得的精子计数的准确性和可靠性是否得到提高;3)在对SS效应进行校正后,确定使用Leja载玻片获得的精子数量是否比使用血细胞计获得的精子数量更有利;4)通过LOA确定这些方法是否可以被认为是可互换的,从而为其常规临床应用提供验证。本研究的目的是确定在生育实验室环境中用于分析精子数量的三种不同方法是否可以被认为是可互换的。这三种方法目前在英国和世界各地的实验室中使用。ICC、CV和CI值表明,所有计数方法都具有特别高的可重复性/可靠性。血细胞计是最可靠的方法,具有最高的ICC,最低的CV和最小的95% CI。这一发现部分支持血细胞计作为金标准方法,尽管其精度显然不高。Leja是第二可靠的方法,尽管没有固定/稀释步骤更可靠,这表明这一步可能会引入一定程度的误差。分析表明,马克勒腔的可靠性明显低于血细胞计或Leja。对于未稀释和稀释的样品,马克勒室的ICC都要低得多,CV和CI在重复计数之间表现出很大的差异。LOA分析表明Leja载玻片可以与血细胞计进行比较,特别是1:1稀释。然而,尽管显示Leja 1:1与血细胞计的平均差为零,但计算出的标准差为0.9。因此,LOA介于- 2.04和1.7之间,这意味着在最坏的情况下,血细胞计中含有5 × 106/mL的标本的精子计数可能在0到16 × 106/mL之间。同样,Leja法可以测定20 × 106个精子/mL样品的浓度在6 × 106和38 × 106个精子/mL之间。虽然后一种分析形式乍一看似乎缺乏精度,但同样的原理可以应用于使用同一腔室的重复计数。换句话说,在大多数情况下,两个试验箱之间的差异并不比使用同一个试验箱进行重复测量差。当精液是有问题的测试液体时,总会有偶尔的异常值,也许更多的异常值,这可能是由于许多因素中的任何一个(例如,高粘度,采样误差,数学误差,稀释误差或腔室缺陷)。在评估方法的一致性和互换性时,必须将其放在期望级别的上下文中。由于使用重复测量或个体之间的血细胞计数存在固有的变异性,因此在将其与其他腔室进行比较时,我们无疑会发现差异。在这种情况下,Leja载玻片可以被视为与血细胞计互换,特别是如果样品首先固定和稀释。所有的结果都非常清楚地表明,应用SS因子增加了Leja计数和血细胞计计数之间的一致性,正如预期的那样。这种改善对于1:1稀释的样品更为明显,对于改进的Leja计数,与血细胞计的平均差异变为0。这是令人放心的,因为Leja指令手册中指出,校正因子最初是通过使用改进的纽鲍尔室校准Leja来计算的。 马克勒试管与所有其他方法的一致性极差,并且有高估精子数量的倾向。在最坏的情况下,20 × 106/mL的样本中可能发现9.2 × 106至58.9 × 106/mL的精子,这可能对诊断或治疗实验室造成严重后果。这一发现支持了先前的研究,即Makler产生高精子数量(Ginsburg和Armant, 1990;Sukcharoen et al ., 1994;Seaman et al, 1996;Coetzee和Menkveld, 2001;Lu et al ., 2004)。实验室提供已知固定浓度为35 × 106精子/mL的乳胶珠溶液,测定Makler上的浓度平均为53.5 × 106/mL。Seaman等人(1996)进行的一项类似的研究发现,Makler实验室将已知的铅浓度高估了50%。使用Leja载玻片测定的计数与使用血细胞计(P <.05),除非他们的标本是先固定和稀释。Leja的中位数明显低于血细胞计的中位数,这一发现得到了LOA分析的支持,该分析表明,Leja在使用未稀释精液时平均低估了精子数量。这种低估在整个数据分布中是一致的,与样本的精子浓度无关。由于Tomlinson等人(2001)的一项研究发现Leja计数明显低于血细胞计,因此预计Leja会低估精子计数(P <0.0001)比相应的血细胞计读数要高,尽管这些计数是使用以前版本的Leja室进行的,并且不知道SS因素。用Makler方法固定和稀释样品进行分析,减少了平均差异,增加了与血细胞计计数的一致程度。然而,无论在未稀释或稀释的标本上进行计数,在Makler腔中产生的计数明显高于血细胞计。在某些情况下,实验室显然愿意在精子参数测量的准确性上做出妥协,以最大限度地提高速度和便利性。在许多情况下,对精子计数方法的偏好和计数室的选择可能反映了临床服务的类型和特定实验室提供的专业知识水平。众所周知,由于方便,许多试管婴儿实验室倾向于一步法,尽管这可能会间接损害实践,因为未来基于精子阈值的治疗决策可能来自错误的数据。以前曾有人提出,使用不同的方法来分析精子浓度是实验室之间精子数量差异的主要原因(Auger等人,2000年)。由于实验室之间的分歧,患者可能被一个实验室分类为正常,而被另一个实验室分类为不育(Neuwinger et al, 1990)。人们早就知道这一点,并得到本研究结果的支持。Leja和血细胞计的精子浓度差异影响了21例患者的诊断。这种错误的诊断可能对患者造成严重后果,其中一些人可能被误诊为不孕症(根据世卫组织的标准),这反过来可能产生负面的社会心理影响,并意味着一些人在实现怀孕方面得不到适当的帮助。我们从以前的研究中知道,目前使用的许多方法都有一定程度的误差,与许多其他类型的诊断测试相比,这是很高的,其中许多是全自动的。简单的因素,如精液固有的黏性和异质性,混合不完全,移液错误,数学和转录,都是有影响的。很可能普遍缺乏共识和缺乏强有力的证据将精子浓度与自然或辅助受孕联系起来,这是由于许多使用的方法的不良实践或固有的不准确性。另一个可能也是最重要的误差来源是抽样误差。就其本质而言,1微升的精液与其他精液相比可能具有非常不同的品质。因此,只有通过更好的混合,增加精液的体积,增加每次分析的精子数量,我们才有希望提高目前的准确性和精密度。但是,这必须与是否需要这种程度的准确性以及它是否能很好地利用资源相权衡。在分析过程中,由于所使用的方法、抽样错误、转录或错误识别的情况,错误的风险相对较高,这就提出了一个问题,即诊断是否应该基于单一精液样本的结果。 再加上其他变量,比如样本是否完整、禁欲的时间长短、疾病、压力和药物,所有这些都已知会影响精子数量,这就确保了男性生育能力和精子数量之间的关系比应有的要弱。不幸的是,精液分析在自然受孕或辅助受孕(如IUI、IVF和ICSI)方面的预测价值仍然很差。血细胞计法长期以来一直是评估精子浓度的公认标准。事实上,世界卫生组织在其精液分析指南(1999)中建议,应该使用血细胞计,如改进的Neubauer,来测量精子浓度。尽管如此,估计有64%的实验室使用血细胞计,26%使用Makler室,其余使用Leja载玻片等替代一次性方法(Keel et al, 2000)。一次性方法,如Leja滑梯,和可重复使用的玻璃室,如Makler,已经被提出作为方便的替代方案。目前的研究表明,所有这些方法之间存在有限的一致性,血细胞测定法和Makler方法之间的差异最大。如果通过固定和稀释样品来修改标准Leja方法,则与血细胞计画法的总体一致性非常好。因此,如果可以证明这两种方法可能给出相同的计数,则可以说这两种方法是可互换的,从而为Leja方法提供了一定程度的验证。血细胞计在精确度方面稍好,但像所有的方法一样,在可靠性和可重复性方面存在内在的弱点,这可能与所讨论的测试液体有关。综上所述,血细胞计和稀释Leja法在平均精子计数方面几乎没有什么不同,这表明Leja玻片可能适合于临床应用。相比之下,Makler方法在整个数据范围内的一致性非常差,不能推荐使用。这三种方法之间的有限一致性以及它们明显缺乏精度令人担忧。如果世界卫生组织继续推荐血球计作为金标准方法,那么至少应该对该方法进行重新评估。检测的不准确常常被归咎于糟糕的技术或技术培训,然而很明显,所有的精子计数方法都有固有的弱点。实验室必须配备更好的设备,以便为其服务的用户(例如,妇产科临床医生)提供服务。提供有关测试的适当信息,包括其局限性和预期的准确性和精确度,以便有效地管理他们的男性患者。
ANDROLOGY LAB CORNER*: Validation of Sperm Counting Methods Using Limits of Agreement
A variety of methods exist for counting sperm. Since the introduction of semen analysis, one of these methods, the hemocytometer, has been regarded as the gold standard by andrology laboratories and the World Health Organization (WHO, 1999). The flexible features of this approach, involving fixation and immobilization of sperm, dilution of highly concentrated samples, and the counting of sperm in a single plane, contribute to the accuracy of the Improved Neubauer hemocytometer and its relative ease of use. This method is strongly accepted within andrology clinics and has been clinically validated by a number of studies (Dunphy et al, 1989; Tomlinson et al, 1996, 1999; Guzick et al, 2001).
As technology and techniques improve, manufacturers are continually trying to develop newer, simpler, quicker and more accurate methods for determining sperm concentration. Busy assisted reproduction technology (ART) laboratories in particular would find a quicker yet comparatively accurate method highly desirable, since sperm counting is an essential part of the semen preparation process. Although modern methods may be faster, since unfixed, undiluted semen is used, some labs find these analyses more difficult to use and believe that the counting of motile sperm may produce erroneous results. Furthermore, the WHO states that the newly introduced methods “are convenient in that they can be used without dilution of the specimen, but that they may lack the accuracy of the hemocytometer technique especially for highly viscous and/or heterogeneous specimens. If such chambers are to be used, their adequate accuracy and precision must be established by comparison with hemocytometers” (WHO, 1999).
In addition, it is now a requirement of laboratory accreditation systems that laboratories provide clinical validation for all methods used (ie, demonstrate that they are “fit for purpose”). Currently, the only sperm counting method with a considerable body of evidence to support and clincally justify its use is the hemocytometer (Mortimer, 1994; WHO, 1999).
When using the hemocytometer, the sperm number is calculated using a fixed volume of semen under the coverslip and counting the sperm in a single plane. A significant association between pregnancy and the sperm concentration measured has consistently been shown for this method (Dunphy et al, 1989; Tomlinson et al, 1996, 1999; Guzick et al, 2001). Thus, 64% of laboratories involved in the analysis of semen use this method routinely (Keel et al, 2000).
However, despite its validity as a method, the use of hemocytometry is thought by many to be inconvenient, in that the hemocytometer must be cleaned and assembled prior to each counting event and it involves the use of dilution techniques that can introduce errors, either due to poor technique or the viscous nature of the semen itself. Mathematical mistakes can occur when applying the correction factor to determine the eventual counts, and the recommended dilution method uses fixatives, such as formal saline, which are often a reason for rejection of the method by embryologists in IVF laboratories.
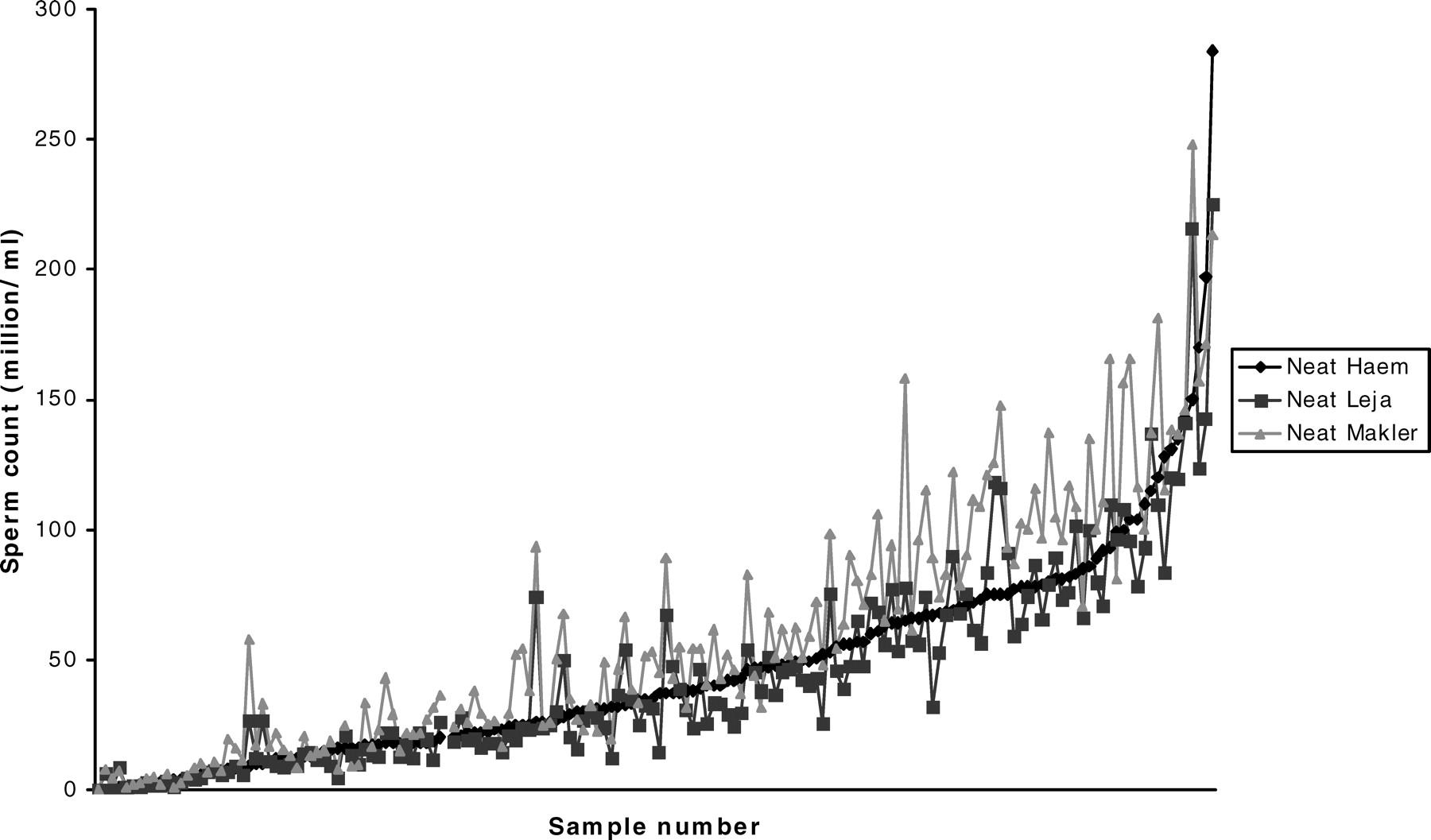
Comparisons of other counting chambers with the hemocytometer, particularly those marketed as easy-to-use 1-step methods have generally not been favorable. Makler sperm counts have been shown to be generally higher than the corresponding counts obtained with the hemocytometer (Coetzee and Menkveld, 2001; Sukcharoen et al, 1994). Indeed, Ginsburg and Armant (1990) have found the Makler chamber counts to be 62% higher than those obtained with the hemocytometer when using latex beads. Other methods, such as the Leja slide (Gynotec Malden, Nieuw-Vennep, The Netherlands) or the Microcell (Conception Technologies, San Diego, Calif) have been shown to produce significantly lower average sperm counts as compared to the hemocytometer. In particular, marked differences were seen at high concentrations (Tomlinson et al, 2001). A number of potential sources of error have been suggested to cause these discrepancies when using 1-step methods. First, the recommendation that motile sperm are counted, which may mean a single spermatozoon is counted more than once or not counted at all. Second and perhaps more significantly is the phenomenum that affects capillary-loaded chambers, such as the Leja and Microcell slides, which is known as the Segre-Silberberg (SS) effect (Segre and Silberberg, 1961). The SS effect results in high-gradient fluid flow in thin capillary-loaded slides, which results in the sperm suspension being forced transversely towards the walls, causing uneven cell dispersion throughout the chamber. New measures have recently been introduced to compensate for this phenomenon. A correction factor is used, which makes allowances for changes in sample viscosity and appears to improve the performance of there slides in terms of agreement with the hemocytometer (Douglas-Hamilton et al, 2005). Third, many of the studies that have compared the performances of various methods with the gold standard of the hemocytometer are problematic in terms of the choice of statistics. Unfortunately, many of these studies have focused on analysing differences across a range of sperm counts, whereas a proper and more detailed analysis is one that compares each and every individual count and measures the agreement between these 2 parameters. Therefore, in the present study, we employ limits of agreement (LoA) to analyse comparative data. This approach, which is based on graphical techniques and simple calculations, allows comparisons between new measurement techniques (ie, the Leja and Makler chambers) and an established method (ie, the hemocytometer). Thus, we can evaluate whether the methods agree sufficiently for the new method to replace the old method and we can decide if the differences between the 2 methods are sufficiently small for the methods to be used interchangeably (Bland and Altman, 1986).
The objectives of the present study were: 1) to determine whether the sperm counts obtained using the Leja slide and Makler chamber compare favorably with the counts obtained using the hemocytometer; 2) to determine whether the accuracy and reliability of sperm counts obtained using the Leja slide and the Makler chamber are improved by prior fixation and dilution of the specimen; 3) to determine whether the sperm counts obtained using the Leja slide compared more favorably with the counts obtained using the hemocytometer when correction is made for the SS effect; and 4) to determine by the use of LOA whether these methods can be considered to be interchangeable, thereby providing validation for their routine clinical application.
The aim of the present investigation was to determine whether three different methods used for analyzing sperm counts in a fertility laboratory setting could be considered to be interchangable. All 3 methods are currently in use in laboratories throughout the United Kingdom and worlwide.
The ICC, CV, and CI values show that all the counting methods have a particularly high degree of repeatability/reliability. The hemocytometer was the most reliable method, with the highest ICC, lowest CV, and smallest 95% CI. This finding partially supports the hemocytometer as the gold standard method, although its precision is clearly not high. The Leja was the next most reliable method, although it was more reliable without the fixation/dilution step, which suggests that this step may introduce a degree of error. The analyses showed the Makler chamber to have significantly poorer reliability than the hemocytometer or Leja. The ICC of the Makler chamber was much lower for both undiluted and diluted samples, and the CV and CI showed great variability between the repeated counts.
The LOA analysis showed that the Leja slide could be compared favourably with the hemocytometer, particularly for the 1:1 dilutions. However, despite showing that the Leja 1:1 and hemocytometer have a mean difference of zero, the standard deviation was calculated as 0.9. Thus, the LOA lie between −2.04 and 1.7, which means that in a worst case scenario, specimens that contain 5 × 106/mL in the hemocytometer could have counts between zero and 16 × 106 sperm/mL. Similarly, the Leja method could determine the concentration of a sample with 20 × 106 sperm/mL to be between 6 × 106 and 38 × 106 sperm/mL. Although the latter form of analysis may at first glance appear to lack precision, the same principle can be applied to repeat counts using the same chamber. In other words, in most cases, the difference between the chambers is no worse than repeated measures using the same chamber. There will always be occasional outliers and perhaps more outliers when semen is the test fluid in question and this could be due to any one of a number of factors (eg, hyperviscosity, sampling error, mathematical error, diluting error or chamber flaws). When assessing the agreement and interchangeability of a method, it has to be put in the context of the level of expectation. As there is innate variability in hemocytometer counts using either repeated measures or between individuals, we will undoubtedly detect differences when comparing this with other chambers. In this context, the Leja slide could be viewed as being interchangeable with the hemocytometer, particularly if the sample is first fixed and diluted.
All of the results show very clearly that applying the SS factor increases the level of agreement between the Leja counts and hemocytometer counts, as expected. This improvement was more pronounced for the 1:1 diluted samples, for which the mean difference with the hemocytometer became 0 for the modified Leja counts. This is reassuring, since the Leja Instruction Manual states that the correction factors were initially calculated by calibrating the Leja with the Improved Neubauer chamber.
The Makler chamber showed extremely poor agreement with all the other methods and had a tendency to overestimate sperm counts. In the worst case, a sample of 20 × 106/mL could be found have between 9.2 × 106 and 58.9 × 106 sperm/mL, which could have serious consequences for the diagnostic or treatment laboratory. This finding supports previous studies that have found that the Makler produces high sperm counts (Ginsburg and Armant, 1990; Sukcharoen et al, 1994; Seaman et al, 1996; Coetzee and Menkveld, 2001; Lu et al, 2004). Laboratories provided with a latex bead solution with a known, fixed concentration of 35 × 106 sperm/mL determined the concentration on the Makler to be 53.5 × 106/mL on average. A similar study conducted by Seaman et al (1996) found that the Makler chamber overestimated the known bead concentrations by as much as 50%.
The counts determined using the Leja slide were significantly different from the counts obtained using the hemocytometer (P < .05), unless they specimens were first fixed and diluted. The Leja median was significantly lower than that of the hemocytometer, and this finding was supported by the LOA analysis, which showed that the Leja on average underestimated the sperm count when undiluted semen was used. This underestimation was consistent throughout the data distribution and was not related to the sperm concentrations of the samples. It was expected that the Leja would underestimate the sperm count when compared to the hemocytometer, since a study by Tomlinson et al (2001) has found Leja counts to be significantly lower (P < .0001) than the corresponding hemocytometer readings, although these counts were performed using a previous version of the Leja chamber and without knowledge of the SS factor.
Fixing and diluting the samples for analysis by the Makler method reduced the mean difference and increased the level of agreement with the hemocytometer counts. However the counts produced in the Makler chamber were significantly higher than those in the hemocytometer, regardless of whether they were performed on undiluted or diluted specimens.
In some instances, laboratories are clearly willing to compromise on the accuracy of sperm parameter measurements in order to maximise speed and convenience. The preference for methods of sperm counting and the selection of counting chambers may in many cases reflect the type of clinical service and the level of expertise provided by a particular laboratory. It is known that many IVF labs favor the 1-step methods owing to their convenience, even though this could indirectly compromise practice, in that future treatment decisions based on sperm thresholds could be derived from erroneous data.
It has been suggested previously that using different methodologies to analyze sperm concentrations is the major cause of variation in sperm counts between laboratories (Auger et al, 2000). Owing to disagreements between laboratories, a patient could be classified as normal by one and as infertile by another (Neuwinger et al, 1990). This has been known for some time and is supported by the findings of the present study. Sperm concentration discrepancies between the Leja and hemocytometer affected the diagnosis of 21 patients in the present study. Such erroneous diagnoses could have serious consequences for patients, some of whom may be misidentified as infertile (according to the WHO criteria), which could in turn have negative psychosocial implications and mean that some individuals would not receive the appropriate assistance in achieving pregnancy.
We know from previous studies that many of the current methods in use carry a degree of error, which is high in comparison with many other types of diagnostic testing, many of which are fully automated. Simple factors, such as the inherent viscosity and heterogeneity of semen, incomplete mixing, errors in pipetting, mathematics, and transcribing, are all contributory. It is likely that the general lack of consensus and lack of strong evidence linking sperm concentration with either natural or assisted conception are due to either poor practice or the intrinsic inaccuracies of many of the methods used.
Another source of error, and possibly the most significant, is sampling error. By its very nature, 1 small microlitre aliquot of semen may have very different qualities when compared to another. Therefore, only by better mixing, increasing the volume of seminal fluid, and increasing the number of sperm counted per analysis can we hope to improve the current degrees of accuracy and precision. However, this has to balanced against whether there is a need for such a degree of accuracy and also whether it is a good use of resources.
The relatively high risk of error during the analysis, be it due to the method used, sampling error, transcription or a case of mistaken identity, raises the question as to whether a diagnosis should ever be based upon the findings of a single semen sample. Adding in other variables, such as whether the sample is complete, length of sexual abstinence, illness, stress, and medications, all of which are known to affect sperm count, ensures that the relationship between male fertility and sperm count is weaker than perhaps it should be. The unfortunate consequence of this is that semen analysis continues to demonstrate poor predictive value in terms of either natural or assisted conception (eg, IUI, IVF, and ICSI).
The hemocytometer method has long been the accepted standard for the assessment of sperm concentration. Indeed, the WHO recommends in its guide to semen analysis (1999) that a hemocytometer, such as the Improved Neubauer, should be used for sperm concentration measurements. Despite this, an estimated 64% of laboratories used the hemocytometer, while 26% used the Makler chamber, and the remainder used alternative disposable methods, such as the Leja slide (Keel et al, 2000). One-step disposable methods, such as the Leja slide, and re-usable glass chambers, such as the Makler, have been put forward as convenient alternatives. The present study suggests that there is limited agreement between all of these methods, with the widest discrepancy between hemocytometry and the Makler method.
If the standard Leja method was modified by fixing and diluting the sample, the overall agreement with hemocytometery was very good. Therefore, if it can be shown that the 2 methods are likely to give the same counts, the 2 methods could be said to be interchangble, providing a degree of validation for the Leja method. The hemocytometer is marginally better in terms of precison but, like all of the methods, has intrinsic weaknesses in terms of reliability and repeatability, which may be related to the test fluid in question.
In conclusion, there is little to choose between the hemocytometer and diluted Leja method in terms of average sperm count, which suggests that the Leja slide may be suitable for use in clinical pactice. In contrast, the Makler method showed very poor agreement throughout the entire data range and cannot be recommended. The limited agreement seen between all 3 methods and their apparent lack of precision is a cause for concern. If the WHO continues to recommend the hemocytometer as the gold standard method, then there should at least be a reappraisal of the method. Testing inaccuracies are often blamed on poor technique or technical training, yet it is clear that all methods for sperm counting have inherent weaknesses. Laboratories must be better equipped in order to provide users of their service (eg, Ob/Gyn clinicians). with proper information about the test, including its limitations and the expected level of accuracy and precision, in order to allow efficient management of their male patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
