Isabel Püntmann, Norbert Schmacke, Arne Melander, Gunnar Lindberg, Bernd Mühlbauer
{"title":"EVITA:用于早期评估药物创新治疗优势的工具。","authors":"Isabel Püntmann, Norbert Schmacke, Arne Melander, Gunnar Lindberg, Bernd Mühlbauer","doi":"10.1186/1472-6904-10-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>New drugs are generally claimed to represent a therapeutic innovation. However, scientific evidence of a substantial clinical advantage is often lacking. This may be the result of using inadequate control groups or surrogate outcomes only in the clinical trials. In view of this, EVITA was developed as a user-friendly transparent tool for the early evaluation of the additional therapeutic value of a new drug.</p><p><strong>Methods: </strong>EVITA does not evaluate a new compound per se but in an approved indication in comparison with existing therapeutic strategies. Placebo as a comparator is accepted only in the absence of an established therapy or if employed in an add-on strategy on top. The evaluation attributes rating points to the drug in question, taking into consideration both therapeutic benefit and risk profile. The compound scores positive points for superiority in efficiency and/or adverse effects as demonstrated in randomized controlled trials (RCTs), whilst negative points are awarded for inferiority and/or an unfavorable risk profile. The evaluation follows an algorithm considering the clinical relevance of the outcomes, the strength of the therapeutic effect and the number of RCTs performed. Categories for therapeutic aim and disease severity, although essential parts of the EVITA assessment, are attributed but do not influence the EVITA score which is presented as a color-coded bar graph. In case the available data were unsuitable for an EVITA calculation, a traffic-type yield sign is assigned instead to criticize such practice. The results are presented online http://www.evita-report.de together with all RCTs considered as well as the reasons for excluding a given RCT from the evaluation. This allows for immediate revision in response to justified criticism and simplifies the inclusion of new data.</p><p><strong>Results: </strong>As examples, four compounds which received approval within the last years were evaluated for one of their clinical indications: lenalidomide, pioglitazone, bupropion and zoledronic acid. Only the first achieved an EVITA score above zero indicating therapeutic advantage.</p><p><strong>Conclusions: </strong>The strength of EVITA appears to lie in its speedy assessment of the potential therapeutic advantage of a new drug for a given indication. At the same time, this approach draws attention to the typical deficits of data used for drug approval. EVITA is not intended to replace classical health technology assessment reports but rather serves as a screening tool in the sense of horizon scanning.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":"10 ","pages":"5"},"PeriodicalIF":0.0000,"publicationDate":"2010-03-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1472-6904-10-5","citationCount":"13","resultStr":"{\"title\":\"EVITA: a tool for the early evaluation of pharmaceutical innovations with regard to therapeutic advantage.\",\"authors\":\"Isabel Püntmann, Norbert Schmacke, Arne Melander, Gunnar Lindberg, Bernd Mühlbauer\",\"doi\":\"10.1186/1472-6904-10-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>New drugs are generally claimed to represent a therapeutic innovation. However, scientific evidence of a substantial clinical advantage is often lacking. This may be the result of using inadequate control groups or surrogate outcomes only in the clinical trials. In view of this, EVITA was developed as a user-friendly transparent tool for the early evaluation of the additional therapeutic value of a new drug.</p><p><strong>Methods: </strong>EVITA does not evaluate a new compound per se but in an approved indication in comparison with existing therapeutic strategies. Placebo as a comparator is accepted only in the absence of an established therapy or if employed in an add-on strategy on top. The evaluation attributes rating points to the drug in question, taking into consideration both therapeutic benefit and risk profile. The compound scores positive points for superiority in efficiency and/or adverse effects as demonstrated in randomized controlled trials (RCTs), whilst negative points are awarded for inferiority and/or an unfavorable risk profile. The evaluation follows an algorithm considering the clinical relevance of the outcomes, the strength of the therapeutic effect and the number of RCTs performed. Categories for therapeutic aim and disease severity, although essential parts of the EVITA assessment, are attributed but do not influence the EVITA score which is presented as a color-coded bar graph. In case the available data were unsuitable for an EVITA calculation, a traffic-type yield sign is assigned instead to criticize such practice. The results are presented online http://www.evita-report.de together with all RCTs considered as well as the reasons for excluding a given RCT from the evaluation. This allows for immediate revision in response to justified criticism and simplifies the inclusion of new data.</p><p><strong>Results: </strong>As examples, four compounds which received approval within the last years were evaluated for one of their clinical indications: lenalidomide, pioglitazone, bupropion and zoledronic acid. Only the first achieved an EVITA score above zero indicating therapeutic advantage.</p><p><strong>Conclusions: </strong>The strength of EVITA appears to lie in its speedy assessment of the potential therapeutic advantage of a new drug for a given indication. At the same time, this approach draws attention to the typical deficits of data used for drug approval. EVITA is not intended to replace classical health technology assessment reports but rather serves as a screening tool in the sense of horizon scanning.</p>\",\"PeriodicalId\":9196,\"journal\":{\"name\":\"BMC Clinical Pharmacology\",\"volume\":\"10 \",\"pages\":\"5\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2010-03-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1472-6904-10-5\",\"citationCount\":\"13\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Clinical Pharmacology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1472-6904-10-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-10-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
EVITA: a tool for the early evaluation of pharmaceutical innovations with regard to therapeutic advantage.
Background: New drugs are generally claimed to represent a therapeutic innovation. However, scientific evidence of a substantial clinical advantage is often lacking. This may be the result of using inadequate control groups or surrogate outcomes only in the clinical trials. In view of this, EVITA was developed as a user-friendly transparent tool for the early evaluation of the additional therapeutic value of a new drug.
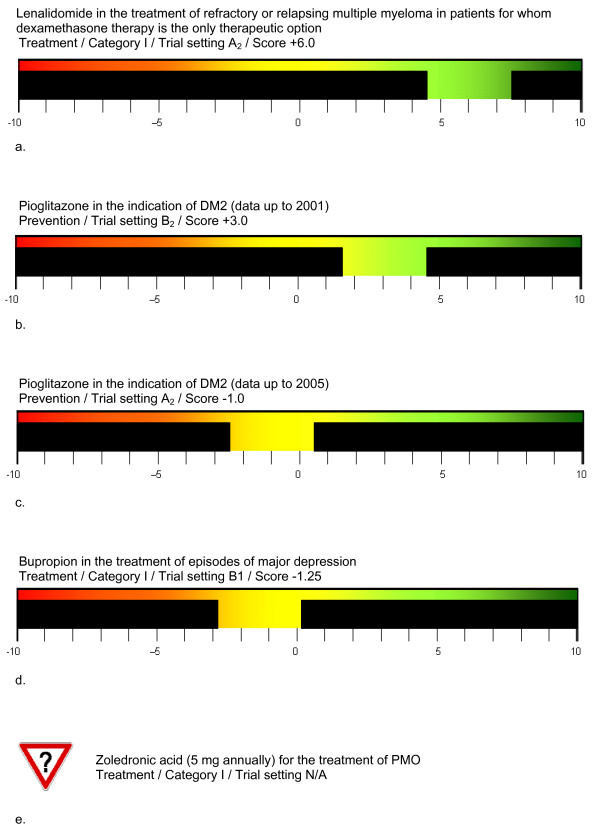
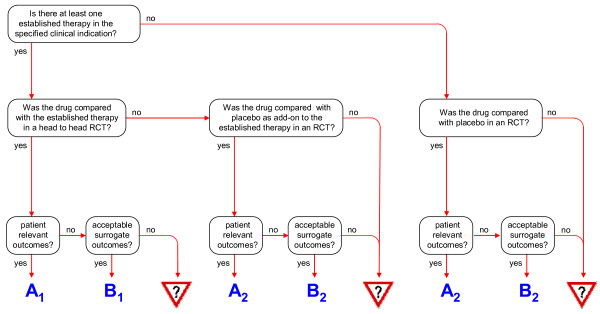
Methods: EVITA does not evaluate a new compound per se but in an approved indication in comparison with existing therapeutic strategies. Placebo as a comparator is accepted only in the absence of an established therapy or if employed in an add-on strategy on top. The evaluation attributes rating points to the drug in question, taking into consideration both therapeutic benefit and risk profile. The compound scores positive points for superiority in efficiency and/or adverse effects as demonstrated in randomized controlled trials (RCTs), whilst negative points are awarded for inferiority and/or an unfavorable risk profile. The evaluation follows an algorithm considering the clinical relevance of the outcomes, the strength of the therapeutic effect and the number of RCTs performed. Categories for therapeutic aim and disease severity, although essential parts of the EVITA assessment, are attributed but do not influence the EVITA score which is presented as a color-coded bar graph. In case the available data were unsuitable for an EVITA calculation, a traffic-type yield sign is assigned instead to criticize such practice. The results are presented online http://www.evita-report.de together with all RCTs considered as well as the reasons for excluding a given RCT from the evaluation. This allows for immediate revision in response to justified criticism and simplifies the inclusion of new data.
Results: As examples, four compounds which received approval within the last years were evaluated for one of their clinical indications: lenalidomide, pioglitazone, bupropion and zoledronic acid. Only the first achieved an EVITA score above zero indicating therapeutic advantage.
Conclusions: The strength of EVITA appears to lie in its speedy assessment of the potential therapeutic advantage of a new drug for a given indication. At the same time, this approach draws attention to the typical deficits of data used for drug approval. EVITA is not intended to replace classical health technology assessment reports but rather serves as a screening tool in the sense of horizon scanning.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
