James M Stocks, Mark L Brantly, Laurene Wang-Smith, Michael A Campos, Kenneth R Chapman, Friedrich Kueppers, Robert A Sandhaus, Charlie Strange, Gerard Turino
{"title":"α 1 -抗胰蛋白酶缺乏症中Prolastin®-C与Prolastin®的药代动力学比较:一项随机研究。","authors":"James M Stocks, Mark L Brantly, Laurene Wang-Smith, Michael A Campos, Kenneth R Chapman, Friedrich Kueppers, Robert A Sandhaus, Charlie Strange, Gerard Turino","doi":"10.1186/1472-6904-10-13","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alpha1-antitrypsin (AAT) deficiency is characterized by low blood levels of alpha1-proteinase inhibitor (alpha₁-PI) and may lead to emphysema. Alpha₁-PI protects pulmonary tissue from damage caused by the action of proteolytic enzymes. Augmentation therapy with Prolastin® (Alpha₁-Proteinase Inhibitor [Human]) to increase the levels of alpha₁-PI has been used to treat individuals with AAT deficiency for over 20 years. Modifications to the Prolastin manufacturing process, incorporating additional purification and pathogen-reduction steps, have led to the development of an alpha₁-PI product, designated Prolastin®-C (Alpha₁-Proteinase inhibitor [Human]). The pharmacokinetic comparability of Prolastin-C to Prolastin was assessed in subjects with AAT deficiency.</p><p><strong>Methods: </strong>In total, 24 subjects were randomized to receive 60 mg/kg of functionally active Prolastin-C or Prolastin by weekly intravenous infusion for 8 weeks before crossover to the alternate treatment for another 8 weeks. Pharmacokinetic plasma samples were drawn over 7 days following last dose in the first treatment period and over 10 days following the last dose in the second period. The primary end point for pharmacokinetic comparability was area under the plasma concentration versus time curve over 7 days post dose (AUC₀₋₇ (days)) of alpha₁-PI determined by potency (functional activity) assay. The crossover phase was followed by an 8-week open-label treatment phase with Prolastin-C only.</p><p><strong>Results: </strong>Mean AUC₀₋₇ (days) was 155.9 versus 152.4 mg*h/mL for Prolastin-C and Prolastin, respectively. The geometric least squares mean ratio of AUC₀₋₇ (days) for Prolastin-C versus Prolastin had a point estimate of 1.03 and a 90% confidence interval of 0.97-1.09, demonstrating pharmacokinetic equivalence between the 2 products. Adverse events were similar for both treatments and occurred at a rate of 0.117 and 0.078 per infusion for Prolastin-C (double-blind treatment phase only) and Prolastin, respectively (p = 0.744). There were no treatment-emergent viral infections in any subject for human immunodeficiency virus, hepatitis B or C, or parvovirus B19 during the course of the study.</p><p><strong>Conclusion: </strong>Prolastin-C demonstrated pharmacokinetic equivalence and a comparable safety profile to Prolastin.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT00295061.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":"10 ","pages":"13"},"PeriodicalIF":0.0000,"publicationDate":"2010-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1472-6904-10-13","citationCount":"35","resultStr":"{\"title\":\"Pharmacokinetic comparability of Prolastin®-C to Prolastin® in alpha₁-antitrypsin deficiency: a randomized study.\",\"authors\":\"James M Stocks, Mark L Brantly, Laurene Wang-Smith, Michael A Campos, Kenneth R Chapman, Friedrich Kueppers, Robert A Sandhaus, Charlie Strange, Gerard Turino\",\"doi\":\"10.1186/1472-6904-10-13\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Alpha1-antitrypsin (AAT) deficiency is characterized by low blood levels of alpha1-proteinase inhibitor (alpha₁-PI) and may lead to emphysema. Alpha₁-PI protects pulmonary tissue from damage caused by the action of proteolytic enzymes. Augmentation therapy with Prolastin® (Alpha₁-Proteinase Inhibitor [Human]) to increase the levels of alpha₁-PI has been used to treat individuals with AAT deficiency for over 20 years. Modifications to the Prolastin manufacturing process, incorporating additional purification and pathogen-reduction steps, have led to the development of an alpha₁-PI product, designated Prolastin®-C (Alpha₁-Proteinase inhibitor [Human]). The pharmacokinetic comparability of Prolastin-C to Prolastin was assessed in subjects with AAT deficiency.</p><p><strong>Methods: </strong>In total, 24 subjects were randomized to receive 60 mg/kg of functionally active Prolastin-C or Prolastin by weekly intravenous infusion for 8 weeks before crossover to the alternate treatment for another 8 weeks. Pharmacokinetic plasma samples were drawn over 7 days following last dose in the first treatment period and over 10 days following the last dose in the second period. The primary end point for pharmacokinetic comparability was area under the plasma concentration versus time curve over 7 days post dose (AUC₀₋₇ (days)) of alpha₁-PI determined by potency (functional activity) assay. The crossover phase was followed by an 8-week open-label treatment phase with Prolastin-C only.</p><p><strong>Results: </strong>Mean AUC₀₋₇ (days) was 155.9 versus 152.4 mg*h/mL for Prolastin-C and Prolastin, respectively. The geometric least squares mean ratio of AUC₀₋₇ (days) for Prolastin-C versus Prolastin had a point estimate of 1.03 and a 90% confidence interval of 0.97-1.09, demonstrating pharmacokinetic equivalence between the 2 products. Adverse events were similar for both treatments and occurred at a rate of 0.117 and 0.078 per infusion for Prolastin-C (double-blind treatment phase only) and Prolastin, respectively (p = 0.744). There were no treatment-emergent viral infections in any subject for human immunodeficiency virus, hepatitis B or C, or parvovirus B19 during the course of the study.</p><p><strong>Conclusion: </strong>Prolastin-C demonstrated pharmacokinetic equivalence and a comparable safety profile to Prolastin.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT00295061.</p>\",\"PeriodicalId\":9196,\"journal\":{\"name\":\"BMC Clinical Pharmacology\",\"volume\":\"10 \",\"pages\":\"13\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2010-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1472-6904-10-13\",\"citationCount\":\"35\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Clinical Pharmacology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1472-6904-10-13\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-10-13","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Pharmacokinetic comparability of Prolastin®-C to Prolastin® in alpha₁-antitrypsin deficiency: a randomized study.
Background: Alpha1-antitrypsin (AAT) deficiency is characterized by low blood levels of alpha1-proteinase inhibitor (alpha₁-PI) and may lead to emphysema. Alpha₁-PI protects pulmonary tissue from damage caused by the action of proteolytic enzymes. Augmentation therapy with Prolastin® (Alpha₁-Proteinase Inhibitor [Human]) to increase the levels of alpha₁-PI has been used to treat individuals with AAT deficiency for over 20 years. Modifications to the Prolastin manufacturing process, incorporating additional purification and pathogen-reduction steps, have led to the development of an alpha₁-PI product, designated Prolastin®-C (Alpha₁-Proteinase inhibitor [Human]). The pharmacokinetic comparability of Prolastin-C to Prolastin was assessed in subjects with AAT deficiency.
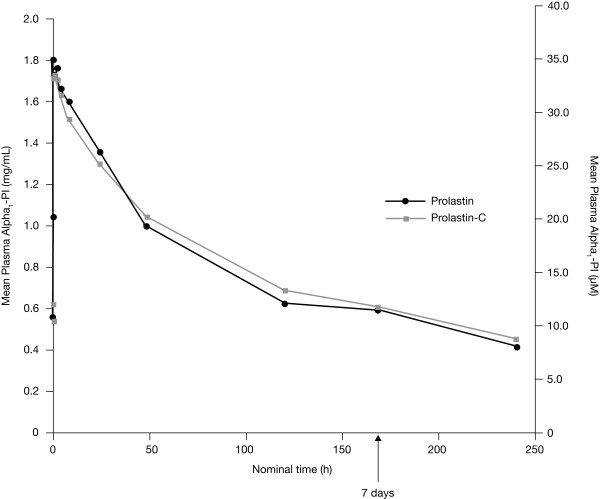
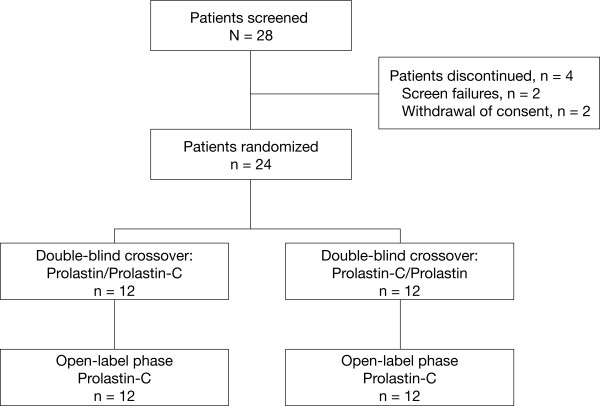
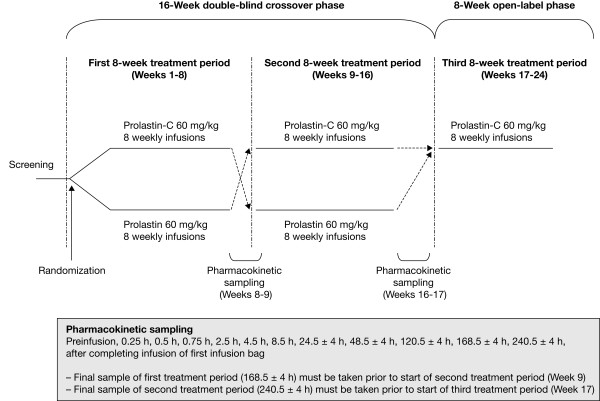
Methods: In total, 24 subjects were randomized to receive 60 mg/kg of functionally active Prolastin-C or Prolastin by weekly intravenous infusion for 8 weeks before crossover to the alternate treatment for another 8 weeks. Pharmacokinetic plasma samples were drawn over 7 days following last dose in the first treatment period and over 10 days following the last dose in the second period. The primary end point for pharmacokinetic comparability was area under the plasma concentration versus time curve over 7 days post dose (AUC₀₋₇ (days)) of alpha₁-PI determined by potency (functional activity) assay. The crossover phase was followed by an 8-week open-label treatment phase with Prolastin-C only.
Results: Mean AUC₀₋₇ (days) was 155.9 versus 152.4 mg*h/mL for Prolastin-C and Prolastin, respectively. The geometric least squares mean ratio of AUC₀₋₇ (days) for Prolastin-C versus Prolastin had a point estimate of 1.03 and a 90% confidence interval of 0.97-1.09, demonstrating pharmacokinetic equivalence between the 2 products. Adverse events were similar for both treatments and occurred at a rate of 0.117 and 0.078 per infusion for Prolastin-C (double-blind treatment phase only) and Prolastin, respectively (p = 0.744). There were no treatment-emergent viral infections in any subject for human immunodeficiency virus, hepatitis B or C, or parvovirus B19 during the course of the study.
Conclusion: Prolastin-C demonstrated pharmacokinetic equivalence and a comparable safety profile to Prolastin.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
