Almath M Spooner, Catherine Deegan, Deirdre M D'Arcy, Caitriona M Gowing, Maria B Donnelly, Owen I Corrigan
{"title":"环丙沙星在危重患者持续静脉-静脉血液渗透中的药代动力学评价。","authors":"Almath M Spooner, Catherine Deegan, Deirdre M D'Arcy, Caitriona M Gowing, Maria B Donnelly, Owen I Corrigan","doi":"10.1186/1472-6904-11-11","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The study aimed to investigate the pharmacokinetics of intravenous ciprofloxacin and the adequacy of 400 mg every 12 hours in critically ill Intensive Care Unit (ICU) patients on continuous veno-venous haemodiafiltration (CVVHDF) with particular reference to the effect of achieved flow rates on drug clearance.</p><p><strong>Methods: </strong>This was an open prospective study conducted in the intensive care unit and research unit of a university teaching hospital. The study population was seven critically ill patients with sepsis requiring CVVHDF. Blood and ultrafiltrate samples were collected and assayed for ciprofloxacin by High Performance Liquid Chromatography (HPLC) to calculate the model independent pharmacokinetic parameters; total body clearance (TBC), half-life (t1/2) and volume of distribution (Vd). CVVHDF was performed at prescribed dialysate rates of 1 or 2 L/hr and ultrafiltration rate of 2 L/hr. The blood flow rate was 200 ml/min, achieved using a Gambro blood pump and Hospal AN69HF haemofilter.</p><p><strong>Results: </strong>Seventeen profiles were obtained. CVVHDF resulted in a median ciprofloxacin t1/2 of 13.8 (range 5.15-39.4) hr, median TBC of 9.90 (range 3.10-13.2) L/hr, a median Vdss of 125 (range 79.5-554) L, a CVVHDF clearance of 2.47+/-0.29 L/hr and a clearance of creatinine (Clcr) of 2.66+/-0.25 L/hr. Thus CVVHDF, at an average flow rate of ~3.5 L/hr, was responsible for removing 26% of ciprofloxacin cleared. At the dose rate of 400 mg every 12 hr, the median estimated Cpmax/MIC and AUC0-24/MIC ratios were 10.3 and 161 respectively (for a MIC of 0.5 mg/L) and exceed the proposed criteria of >10 for Cpmax/MIC and > 100 for AUC0-24/MIC. There was a suggestion towards increased ciprofloxacin clearance by CVVHDF with increasing effluent flow rate.</p><p><strong>Conclusions: </strong>Given the growing microbial resistance to ciprofloxacin our results suggest that a dose rate of 400 mg every 12 hr, may be necessary to achieve the desired pharmacokinetic-pharmacodynamic (PK-PD) goals in patients on CVVHDF, however an extended interval may be required if there is concomitant hepatic impairment. A correlation between ciprofloxacin clearance due to CVVHDF and creatinine clearance by the filter was observed (r2 = 0.76), providing a useful clinical surrogate marker for ciprofloxacin clearance within the range studied.</p><p><strong>Trial registration: </strong>Current Controlled Trials ISRCTN52722850.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":"11 ","pages":"11"},"PeriodicalIF":0.0000,"publicationDate":"2011-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1472-6904-11-11","citationCount":"27","resultStr":"{\"title\":\"An evaluation of ciprofloxacin pharmacokinetics in critically ill patients undergoing continuous veno-venous haemodiafiltration.\",\"authors\":\"Almath M Spooner, Catherine Deegan, Deirdre M D'Arcy, Caitriona M Gowing, Maria B Donnelly, Owen I Corrigan\",\"doi\":\"10.1186/1472-6904-11-11\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The study aimed to investigate the pharmacokinetics of intravenous ciprofloxacin and the adequacy of 400 mg every 12 hours in critically ill Intensive Care Unit (ICU) patients on continuous veno-venous haemodiafiltration (CVVHDF) with particular reference to the effect of achieved flow rates on drug clearance.</p><p><strong>Methods: </strong>This was an open prospective study conducted in the intensive care unit and research unit of a university teaching hospital. The study population was seven critically ill patients with sepsis requiring CVVHDF. Blood and ultrafiltrate samples were collected and assayed for ciprofloxacin by High Performance Liquid Chromatography (HPLC) to calculate the model independent pharmacokinetic parameters; total body clearance (TBC), half-life (t1/2) and volume of distribution (Vd). CVVHDF was performed at prescribed dialysate rates of 1 or 2 L/hr and ultrafiltration rate of 2 L/hr. The blood flow rate was 200 ml/min, achieved using a Gambro blood pump and Hospal AN69HF haemofilter.</p><p><strong>Results: </strong>Seventeen profiles were obtained. CVVHDF resulted in a median ciprofloxacin t1/2 of 13.8 (range 5.15-39.4) hr, median TBC of 9.90 (range 3.10-13.2) L/hr, a median Vdss of 125 (range 79.5-554) L, a CVVHDF clearance of 2.47+/-0.29 L/hr and a clearance of creatinine (Clcr) of 2.66+/-0.25 L/hr. Thus CVVHDF, at an average flow rate of ~3.5 L/hr, was responsible for removing 26% of ciprofloxacin cleared. At the dose rate of 400 mg every 12 hr, the median estimated Cpmax/MIC and AUC0-24/MIC ratios were 10.3 and 161 respectively (for a MIC of 0.5 mg/L) and exceed the proposed criteria of >10 for Cpmax/MIC and > 100 for AUC0-24/MIC. There was a suggestion towards increased ciprofloxacin clearance by CVVHDF with increasing effluent flow rate.</p><p><strong>Conclusions: </strong>Given the growing microbial resistance to ciprofloxacin our results suggest that a dose rate of 400 mg every 12 hr, may be necessary to achieve the desired pharmacokinetic-pharmacodynamic (PK-PD) goals in patients on CVVHDF, however an extended interval may be required if there is concomitant hepatic impairment. A correlation between ciprofloxacin clearance due to CVVHDF and creatinine clearance by the filter was observed (r2 = 0.76), providing a useful clinical surrogate marker for ciprofloxacin clearance within the range studied.</p><p><strong>Trial registration: </strong>Current Controlled Trials ISRCTN52722850.</p>\",\"PeriodicalId\":9196,\"journal\":{\"name\":\"BMC Clinical Pharmacology\",\"volume\":\"11 \",\"pages\":\"11\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1472-6904-11-11\",\"citationCount\":\"27\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Clinical Pharmacology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1472-6904-11-11\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-11-11","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
An evaluation of ciprofloxacin pharmacokinetics in critically ill patients undergoing continuous veno-venous haemodiafiltration.
Background: The study aimed to investigate the pharmacokinetics of intravenous ciprofloxacin and the adequacy of 400 mg every 12 hours in critically ill Intensive Care Unit (ICU) patients on continuous veno-venous haemodiafiltration (CVVHDF) with particular reference to the effect of achieved flow rates on drug clearance.
Methods: This was an open prospective study conducted in the intensive care unit and research unit of a university teaching hospital. The study population was seven critically ill patients with sepsis requiring CVVHDF. Blood and ultrafiltrate samples were collected and assayed for ciprofloxacin by High Performance Liquid Chromatography (HPLC) to calculate the model independent pharmacokinetic parameters; total body clearance (TBC), half-life (t1/2) and volume of distribution (Vd). CVVHDF was performed at prescribed dialysate rates of 1 or 2 L/hr and ultrafiltration rate of 2 L/hr. The blood flow rate was 200 ml/min, achieved using a Gambro blood pump and Hospal AN69HF haemofilter.
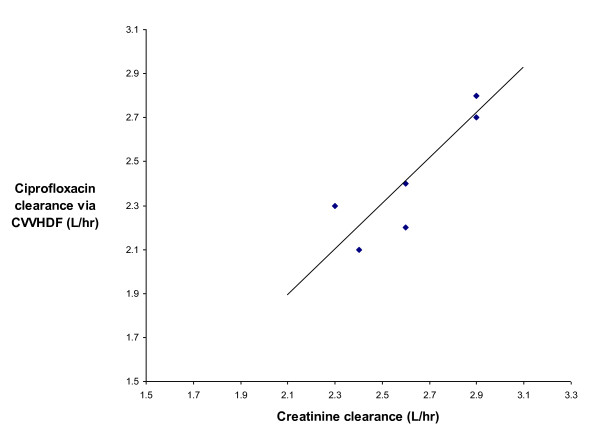
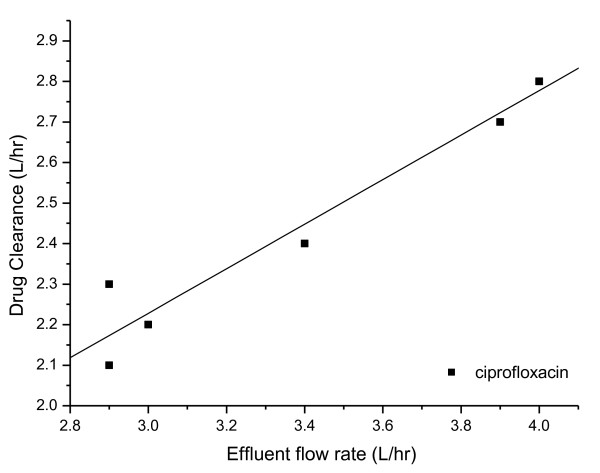
Results: Seventeen profiles were obtained. CVVHDF resulted in a median ciprofloxacin t1/2 of 13.8 (range 5.15-39.4) hr, median TBC of 9.90 (range 3.10-13.2) L/hr, a median Vdss of 125 (range 79.5-554) L, a CVVHDF clearance of 2.47+/-0.29 L/hr and a clearance of creatinine (Clcr) of 2.66+/-0.25 L/hr. Thus CVVHDF, at an average flow rate of ~3.5 L/hr, was responsible for removing 26% of ciprofloxacin cleared. At the dose rate of 400 mg every 12 hr, the median estimated Cpmax/MIC and AUC0-24/MIC ratios were 10.3 and 161 respectively (for a MIC of 0.5 mg/L) and exceed the proposed criteria of >10 for Cpmax/MIC and > 100 for AUC0-24/MIC. There was a suggestion towards increased ciprofloxacin clearance by CVVHDF with increasing effluent flow rate.
Conclusions: Given the growing microbial resistance to ciprofloxacin our results suggest that a dose rate of 400 mg every 12 hr, may be necessary to achieve the desired pharmacokinetic-pharmacodynamic (PK-PD) goals in patients on CVVHDF, however an extended interval may be required if there is concomitant hepatic impairment. A correlation between ciprofloxacin clearance due to CVVHDF and creatinine clearance by the filter was observed (r2 = 0.76), providing a useful clinical surrogate marker for ciprofloxacin clearance within the range studied.
Trial registration: Current Controlled Trials ISRCTN52722850.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
