Jeong Eun Kim, Dok Hyun Yoon, Shin Kim, Dae Ho Lee, Jeong Hoon Kim, Young Hee Yoon, Hyun Sook Chi, Sang Wook Lee, Chan-Sik Park, Jooryung Huh, Cheolwon Suh
{"title":"原发性中枢神经系统淋巴瘤患者复发模式及预后因素分析。","authors":"Jeong Eun Kim, Dok Hyun Yoon, Shin Kim, Dae Ho Lee, Jeong Hoon Kim, Young Hee Yoon, Hyun Sook Chi, Sang Wook Lee, Chan-Sik Park, Jooryung Huh, Cheolwon Suh","doi":"10.5045/kjh.2012.47.1.60","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Primary central nervous system lymphoma (PCNSL) rarely relapses in extracranial sites, and no specialized guidelines for follow-up evaluation have been proposed.</p><p><strong>Methods: </strong>We analyzed 65 patients with newly diagnosed PNCSL to evaluate the pattern of relapse and prognostic factors.</p><p><strong>Results: </strong>Of the 65 patients analyzed, 55 had only parenchymal brain disease, and 10 had both intracranial and extracranial lesions. As a first-line treatment, 29 patients received chemotherapy only (CTx), 13 received chemotherapy followed by whole brain radiotherapy (CTx-WBRT), 18 received chemotherapy followed by autologous stem cell transplantation (CTx-ASCT), 2 received palliative WBRT, and 3 received best supportive care. The overall response rate to the initial treatment was 75.8%, with specific response rates of 62.1% to CTx, 84.6% to CTx-WBRT, and 100% to CTx-ASCT. The complete response (CR) rate was higher with CTx-ASCT than in the absence of ASCT (77.8% vs. 43.2%; P=0.025). After a median follow-up of 18.8 months, the median failure-free survival (FFS) and overall survival (OS) were 13.0 and 36.1 months, respectively. No systemic relapse without a CNS lesion was noted. Multivariate analysis showed that ASCT was predictive of better FFS but not of OS. Age and the Memorial-Sloan Kettering Cancer Center prognostic score were predictive of survival.</p><p><strong>Conclusion: </strong>We observed no systemic relapse without a CNS lesion, suggesting that regular systematic evaluation of extracranial sites may not always be necessary. Age was prognostic of survival irrespective of treatment scheme. ASCT may improve CR rate and FFS.</p>","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"47 1","pages":"60-6"},"PeriodicalIF":0.0000,"publicationDate":"2012-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2012.47.1.60","citationCount":"18","resultStr":"{\"title\":\"Relapse pattern and prognostic factors for patients with primary central nervous system lymphoma.\",\"authors\":\"Jeong Eun Kim, Dok Hyun Yoon, Shin Kim, Dae Ho Lee, Jeong Hoon Kim, Young Hee Yoon, Hyun Sook Chi, Sang Wook Lee, Chan-Sik Park, Jooryung Huh, Cheolwon Suh\",\"doi\":\"10.5045/kjh.2012.47.1.60\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Primary central nervous system lymphoma (PCNSL) rarely relapses in extracranial sites, and no specialized guidelines for follow-up evaluation have been proposed.</p><p><strong>Methods: </strong>We analyzed 65 patients with newly diagnosed PNCSL to evaluate the pattern of relapse and prognostic factors.</p><p><strong>Results: </strong>Of the 65 patients analyzed, 55 had only parenchymal brain disease, and 10 had both intracranial and extracranial lesions. As a first-line treatment, 29 patients received chemotherapy only (CTx), 13 received chemotherapy followed by whole brain radiotherapy (CTx-WBRT), 18 received chemotherapy followed by autologous stem cell transplantation (CTx-ASCT), 2 received palliative WBRT, and 3 received best supportive care. The overall response rate to the initial treatment was 75.8%, with specific response rates of 62.1% to CTx, 84.6% to CTx-WBRT, and 100% to CTx-ASCT. The complete response (CR) rate was higher with CTx-ASCT than in the absence of ASCT (77.8% vs. 43.2%; P=0.025). After a median follow-up of 18.8 months, the median failure-free survival (FFS) and overall survival (OS) were 13.0 and 36.1 months, respectively. No systemic relapse without a CNS lesion was noted. Multivariate analysis showed that ASCT was predictive of better FFS but not of OS. Age and the Memorial-Sloan Kettering Cancer Center prognostic score were predictive of survival.</p><p><strong>Conclusion: </strong>We observed no systemic relapse without a CNS lesion, suggesting that regular systematic evaluation of extracranial sites may not always be necessary. Age was prognostic of survival irrespective of treatment scheme. ASCT may improve CR rate and FFS.</p>\",\"PeriodicalId\":23001,\"journal\":{\"name\":\"The Korean Journal of Hematology\",\"volume\":\"47 1\",\"pages\":\"60-6\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5045/kjh.2012.47.1.60\",\"citationCount\":\"18\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/kjh.2012.47.1.60\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/3/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2012.47.1.60","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/3/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Relapse pattern and prognostic factors for patients with primary central nervous system lymphoma.
Background: Primary central nervous system lymphoma (PCNSL) rarely relapses in extracranial sites, and no specialized guidelines for follow-up evaluation have been proposed.
Methods: We analyzed 65 patients with newly diagnosed PNCSL to evaluate the pattern of relapse and prognostic factors.
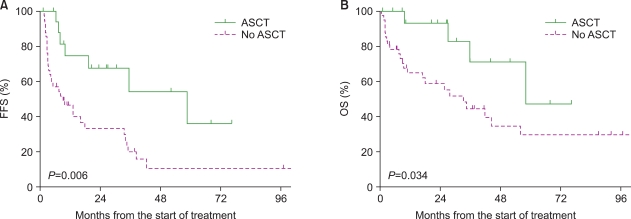
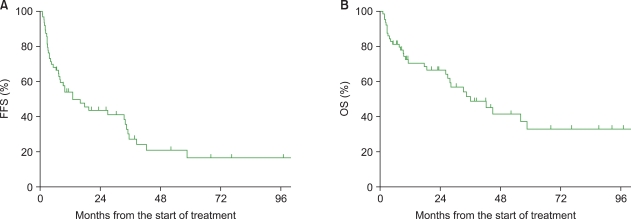
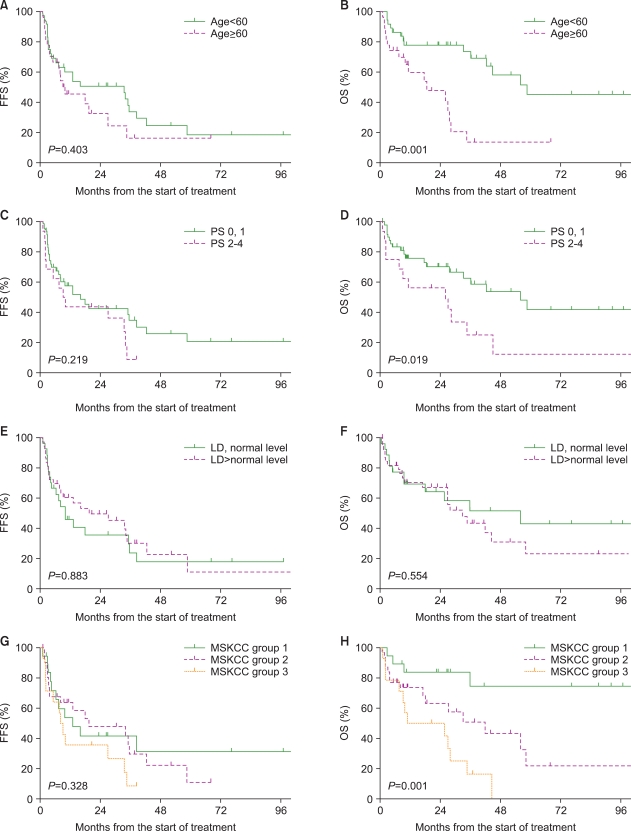
Results: Of the 65 patients analyzed, 55 had only parenchymal brain disease, and 10 had both intracranial and extracranial lesions. As a first-line treatment, 29 patients received chemotherapy only (CTx), 13 received chemotherapy followed by whole brain radiotherapy (CTx-WBRT), 18 received chemotherapy followed by autologous stem cell transplantation (CTx-ASCT), 2 received palliative WBRT, and 3 received best supportive care. The overall response rate to the initial treatment was 75.8%, with specific response rates of 62.1% to CTx, 84.6% to CTx-WBRT, and 100% to CTx-ASCT. The complete response (CR) rate was higher with CTx-ASCT than in the absence of ASCT (77.8% vs. 43.2%; P=0.025). After a median follow-up of 18.8 months, the median failure-free survival (FFS) and overall survival (OS) were 13.0 and 36.1 months, respectively. No systemic relapse without a CNS lesion was noted. Multivariate analysis showed that ASCT was predictive of better FFS but not of OS. Age and the Memorial-Sloan Kettering Cancer Center prognostic score were predictive of survival.
Conclusion: We observed no systemic relapse without a CNS lesion, suggesting that regular systematic evaluation of extracranial sites may not always be necessary. Age was prognostic of survival irrespective of treatment scheme. ASCT may improve CR rate and FFS.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
