{"title":"他克莫司和小剂量甲氨蝶呤预防儿童异基因造血干细胞移植后急性移植物抗宿主病的有效性:韩国单中心研究","authors":"Seong Shik Park, So Eun Jun, Young Tak Lim","doi":"10.5045/kjh.2012.47.2.113","DOIUrl":null,"url":null,"abstract":"Background Knowledge of the roles of tacrolimus and minidose methotrexate (MTX) in the prevention of acute graft-versus-host disease (aGVHD) in pediatric allogeneic hematopoietic stem cell transplantation (HSCT) is limited. We retrospectively evaluated the engraftment status, incidence of aGVHD and chronic GVHD (cGVHD), and toxicities of tacrolimus and minidose MTX in aGVHD prophylaxis in children undergoing allogeneic HSCT. Methods Seventeen children, who underwent allogeneic HSCT and received tacrolimus and minidose MTX as GVHD prophylaxis from March 2003 to February 2011, were reviewed retrospectively. All the patients received tacrolimus since the day before transplantation at a dose of 0.03 mg/kg/day and MTX at a dose of 5 mg/m2 on days 1, 3, 6, and 11. Results Of the 17 patients, 9 received human leukocyte antigen (HLA)-matched related donor transplants, and 8 received HLA-matched, or partially mismatched unrelated donor transplants. The median time for follow-up was 55 months. The incidence of aGVHD in the related and unrelated donor groups was 22.2% and 42.9%, respectively. cGVHD was not observed. To maintain therapeutic blood levels of tacrolimus, the younger group (<8 years of age) required an increased mean dose compared to the older group (≥8 years) (P=0.0075). The adverse events commonly associated with tacrolimus included hypomagnesemia (88%), nephrotoxicity (23%), and hyperglycemia (23%). Conclusion Tacrolimus and minidose MTX were well tolerated and effective in GVHD prophylaxis in pediatric patients undergoing allogeneic HSCT. Children <8 years of age undergoing HSCT required increased doses of tacrolimus to achieve therapeutic levels.","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"47 2","pages":"113-8"},"PeriodicalIF":0.0000,"publicationDate":"2012-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2012.47.2.113","citationCount":"5","resultStr":"{\"title\":\"The effectiveness of tacrolimus and minidose methotrexate in the prevention of acute graft-versus-host disease following allogeneic hematopoietic stem cell transplantation in children: a single-center study in Korea.\",\"authors\":\"Seong Shik Park, So Eun Jun, Young Tak Lim\",\"doi\":\"10.5045/kjh.2012.47.2.113\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Background Knowledge of the roles of tacrolimus and minidose methotrexate (MTX) in the prevention of acute graft-versus-host disease (aGVHD) in pediatric allogeneic hematopoietic stem cell transplantation (HSCT) is limited. We retrospectively evaluated the engraftment status, incidence of aGVHD and chronic GVHD (cGVHD), and toxicities of tacrolimus and minidose MTX in aGVHD prophylaxis in children undergoing allogeneic HSCT. Methods Seventeen children, who underwent allogeneic HSCT and received tacrolimus and minidose MTX as GVHD prophylaxis from March 2003 to February 2011, were reviewed retrospectively. All the patients received tacrolimus since the day before transplantation at a dose of 0.03 mg/kg/day and MTX at a dose of 5 mg/m2 on days 1, 3, 6, and 11. Results Of the 17 patients, 9 received human leukocyte antigen (HLA)-matched related donor transplants, and 8 received HLA-matched, or partially mismatched unrelated donor transplants. The median time for follow-up was 55 months. The incidence of aGVHD in the related and unrelated donor groups was 22.2% and 42.9%, respectively. cGVHD was not observed. To maintain therapeutic blood levels of tacrolimus, the younger group (<8 years of age) required an increased mean dose compared to the older group (≥8 years) (P=0.0075). The adverse events commonly associated with tacrolimus included hypomagnesemia (88%), nephrotoxicity (23%), and hyperglycemia (23%). Conclusion Tacrolimus and minidose MTX were well tolerated and effective in GVHD prophylaxis in pediatric patients undergoing allogeneic HSCT. Children <8 years of age undergoing HSCT required increased doses of tacrolimus to achieve therapeutic levels.\",\"PeriodicalId\":23001,\"journal\":{\"name\":\"The Korean Journal of Hematology\",\"volume\":\"47 2\",\"pages\":\"113-8\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5045/kjh.2012.47.2.113\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/kjh.2012.47.2.113\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/6/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2012.47.2.113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/6/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
The effectiveness of tacrolimus and minidose methotrexate in the prevention of acute graft-versus-host disease following allogeneic hematopoietic stem cell transplantation in children: a single-center study in Korea.
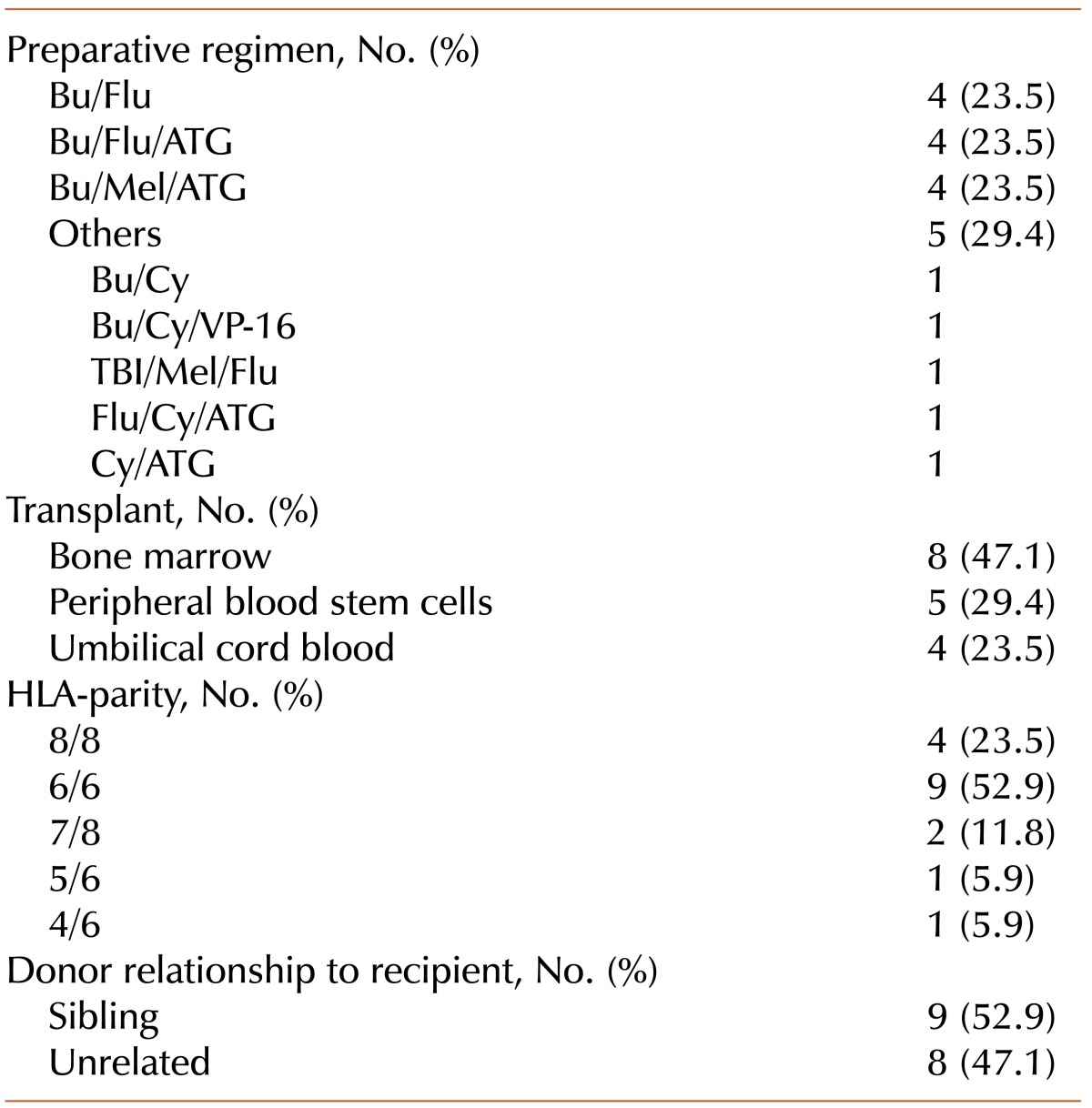
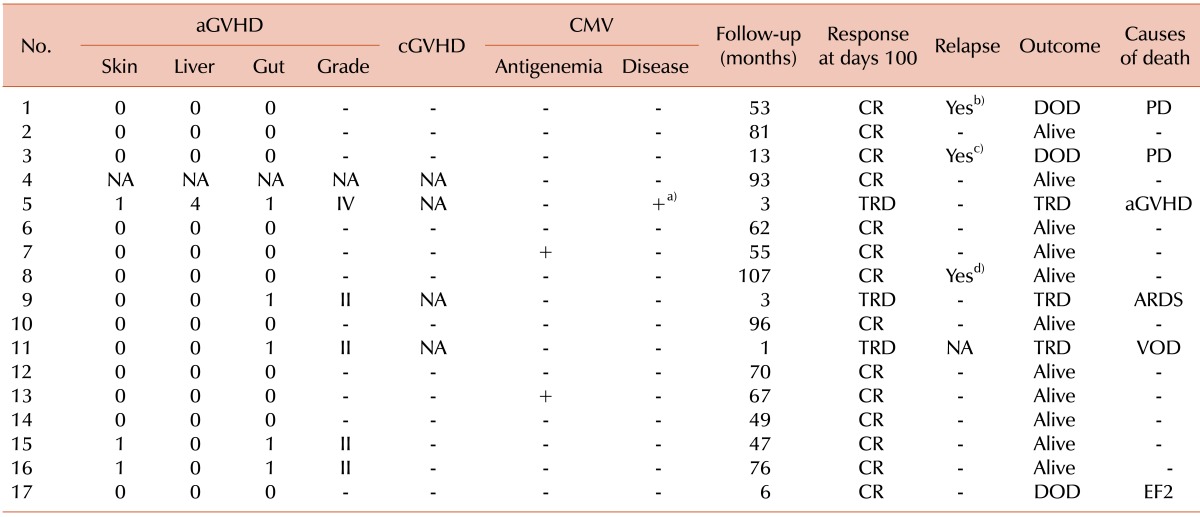
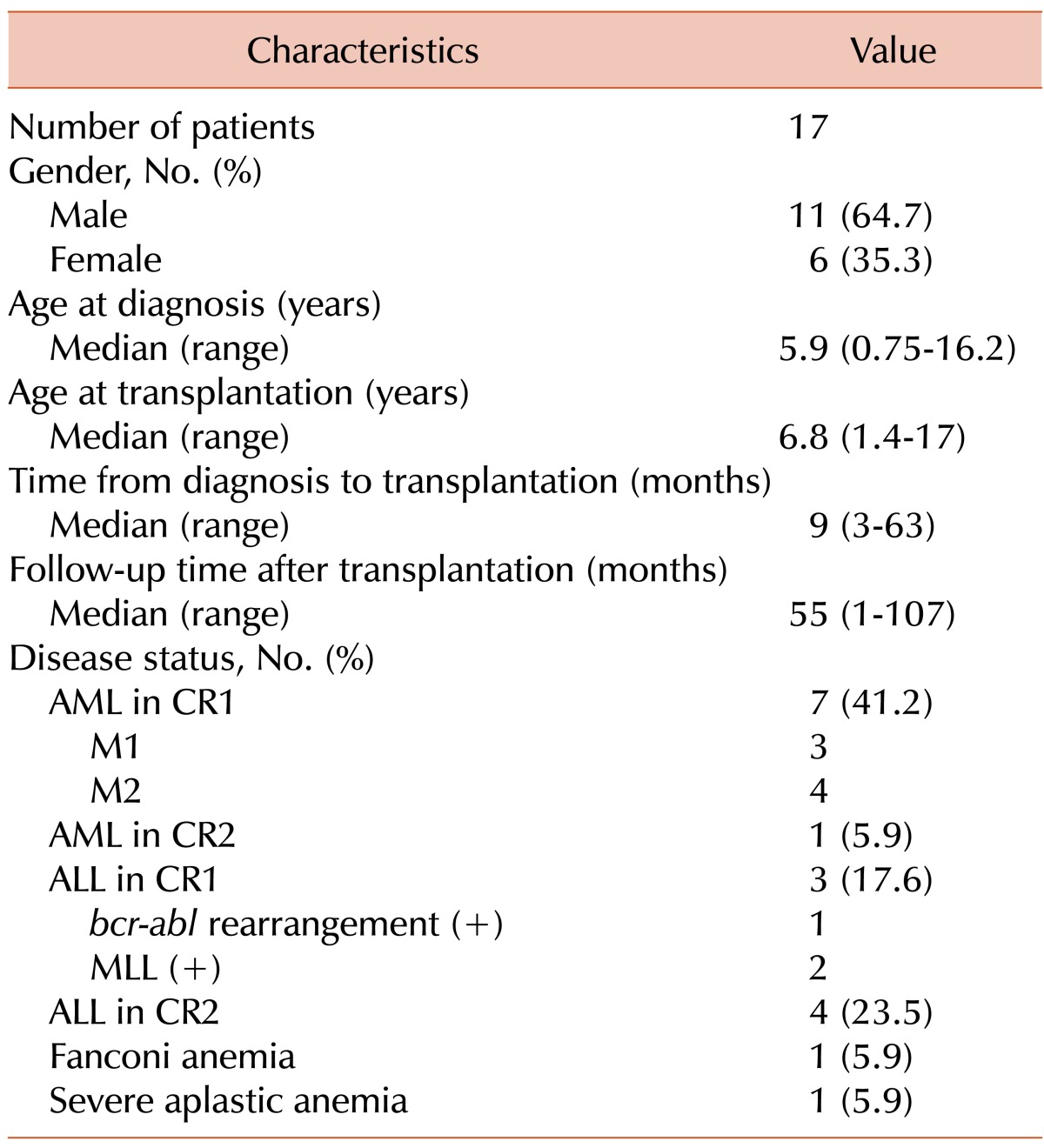
Background Knowledge of the roles of tacrolimus and minidose methotrexate (MTX) in the prevention of acute graft-versus-host disease (aGVHD) in pediatric allogeneic hematopoietic stem cell transplantation (HSCT) is limited. We retrospectively evaluated the engraftment status, incidence of aGVHD and chronic GVHD (cGVHD), and toxicities of tacrolimus and minidose MTX in aGVHD prophylaxis in children undergoing allogeneic HSCT. Methods Seventeen children, who underwent allogeneic HSCT and received tacrolimus and minidose MTX as GVHD prophylaxis from March 2003 to February 2011, were reviewed retrospectively. All the patients received tacrolimus since the day before transplantation at a dose of 0.03 mg/kg/day and MTX at a dose of 5 mg/m2 on days 1, 3, 6, and 11. Results Of the 17 patients, 9 received human leukocyte antigen (HLA)-matched related donor transplants, and 8 received HLA-matched, or partially mismatched unrelated donor transplants. The median time for follow-up was 55 months. The incidence of aGVHD in the related and unrelated donor groups was 22.2% and 42.9%, respectively. cGVHD was not observed. To maintain therapeutic blood levels of tacrolimus, the younger group (<8 years of age) required an increased mean dose compared to the older group (≥8 years) (P=0.0075). The adverse events commonly associated with tacrolimus included hypomagnesemia (88%), nephrotoxicity (23%), and hyperglycemia (23%). Conclusion Tacrolimus and minidose MTX were well tolerated and effective in GVHD prophylaxis in pediatric patients undergoing allogeneic HSCT. Children <8 years of age undergoing HSCT required increased doses of tacrolimus to achieve therapeutic levels.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
