Andrea Messori, Valeria Fadda, Roberta Gatto, Dario Maratea, Sabrina Trippoli
{"title":"急性冠状动脉综合征中的新型口服抗凝剂:与现有疗法相比是否有优势?","authors":"Andrea Messori, Valeria Fadda, Roberta Gatto, Dario Maratea, Sabrina Trippoli","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>After an acute coronary syndrome, dual antiplatelet therapy with clopidogrel plus aspirin is still a standard of care, but several new approaches have been investigated.</p><p><strong>Objectives: </strong>The present study re-examined the studies published thus far on this topic to evaluate the effectiveness of dual antiplatelet therapy in comparison to some of these new approaches (mainly, ticagrelor + aspirin and dual therapy plus a new oral anticoagulant [NOAC]; i.e., \"triple therapy\").</p><p><strong>Materials and methods: </strong>The clinical material was directly derived from that reported in recent meta-analyses. Our re-analysis relied on standard equivalence methods in which interpretation is based on Relative Risks (RRs) along with their 95% Confidence Intervals (CI). The equivalence margins employed in our statistical testing were directly derived from those reported in randomized studies.</p><p><strong>Results: </strong>The equivalence margins were initially set at RR ranging from 0.775 to 1.29. According to these margins, triple therapy based on any NOAC proved to be superior to dual therapy alone, but at the same time demonstrated its equivalence with dual therapy. The results for apixaban-based triple therapy were inconclusive (not superior, not not-inferior, not equivalent and, of course, not inferior to the controls). Those for rivaroxaban-based triple therapy showed that this combination treatment was superior to dual therapy alone and failed to meet the criterion of equivalence. In the comparison between rivaroxaban-based triple therapy and ticagrelor + aspirin, the RR was 1 and its 95% CI remained within a post-hoc margin of ± 15%.</p><p><strong>Conclusions: </strong>Even if one considers the most effective NOAC in combination with clopidogrel + ticagrelor, this triple therapy is not more effective than ticagrelor + aspirin. On the other hand, the increased risk of bleeding with triple regimens is well demonstrated. We therefore conclude that these triple regimens did not play any important roles in the patients experiencing an acute coronary syndrome.</p>","PeriodicalId":43653,"journal":{"name":"International Cardiovascular Research Journal","volume":"8 3","pages":"124-6"},"PeriodicalIF":0.1000,"publicationDate":"2014-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4109037/pdf/","citationCount":"0","resultStr":"{\"title\":\"New oral anticoagulants in acute coronary syndrome: is there any advantage over existing treatments?\",\"authors\":\"Andrea Messori, Valeria Fadda, Roberta Gatto, Dario Maratea, Sabrina Trippoli\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>After an acute coronary syndrome, dual antiplatelet therapy with clopidogrel plus aspirin is still a standard of care, but several new approaches have been investigated.</p><p><strong>Objectives: </strong>The present study re-examined the studies published thus far on this topic to evaluate the effectiveness of dual antiplatelet therapy in comparison to some of these new approaches (mainly, ticagrelor + aspirin and dual therapy plus a new oral anticoagulant [NOAC]; i.e., \\\"triple therapy\\\").</p><p><strong>Materials and methods: </strong>The clinical material was directly derived from that reported in recent meta-analyses. Our re-analysis relied on standard equivalence methods in which interpretation is based on Relative Risks (RRs) along with their 95% Confidence Intervals (CI). The equivalence margins employed in our statistical testing were directly derived from those reported in randomized studies.</p><p><strong>Results: </strong>The equivalence margins were initially set at RR ranging from 0.775 to 1.29. According to these margins, triple therapy based on any NOAC proved to be superior to dual therapy alone, but at the same time demonstrated its equivalence with dual therapy. The results for apixaban-based triple therapy were inconclusive (not superior, not not-inferior, not equivalent and, of course, not inferior to the controls). Those for rivaroxaban-based triple therapy showed that this combination treatment was superior to dual therapy alone and failed to meet the criterion of equivalence. In the comparison between rivaroxaban-based triple therapy and ticagrelor + aspirin, the RR was 1 and its 95% CI remained within a post-hoc margin of ± 15%.</p><p><strong>Conclusions: </strong>Even if one considers the most effective NOAC in combination with clopidogrel + ticagrelor, this triple therapy is not more effective than ticagrelor + aspirin. On the other hand, the increased risk of bleeding with triple regimens is well demonstrated. We therefore conclude that these triple regimens did not play any important roles in the patients experiencing an acute coronary syndrome.</p>\",\"PeriodicalId\":43653,\"journal\":{\"name\":\"International Cardiovascular Research Journal\",\"volume\":\"8 3\",\"pages\":\"124-6\"},\"PeriodicalIF\":0.1000,\"publicationDate\":\"2014-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4109037/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Cardiovascular Research Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Cardiovascular Research Journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
New oral anticoagulants in acute coronary syndrome: is there any advantage over existing treatments?
Background: After an acute coronary syndrome, dual antiplatelet therapy with clopidogrel plus aspirin is still a standard of care, but several new approaches have been investigated.
Objectives: The present study re-examined the studies published thus far on this topic to evaluate the effectiveness of dual antiplatelet therapy in comparison to some of these new approaches (mainly, ticagrelor + aspirin and dual therapy plus a new oral anticoagulant [NOAC]; i.e., "triple therapy").
Materials and methods: The clinical material was directly derived from that reported in recent meta-analyses. Our re-analysis relied on standard equivalence methods in which interpretation is based on Relative Risks (RRs) along with their 95% Confidence Intervals (CI). The equivalence margins employed in our statistical testing were directly derived from those reported in randomized studies.
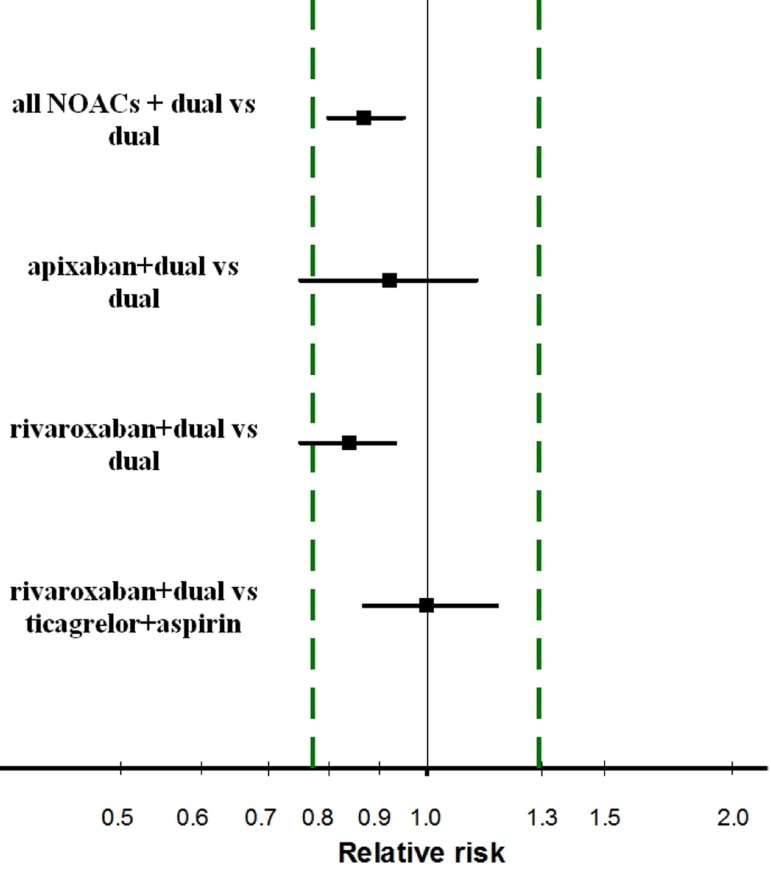
Results: The equivalence margins were initially set at RR ranging from 0.775 to 1.29. According to these margins, triple therapy based on any NOAC proved to be superior to dual therapy alone, but at the same time demonstrated its equivalence with dual therapy. The results for apixaban-based triple therapy were inconclusive (not superior, not not-inferior, not equivalent and, of course, not inferior to the controls). Those for rivaroxaban-based triple therapy showed that this combination treatment was superior to dual therapy alone and failed to meet the criterion of equivalence. In the comparison between rivaroxaban-based triple therapy and ticagrelor + aspirin, the RR was 1 and its 95% CI remained within a post-hoc margin of ± 15%.
Conclusions: Even if one considers the most effective NOAC in combination with clopidogrel + ticagrelor, this triple therapy is not more effective than ticagrelor + aspirin. On the other hand, the increased risk of bleeding with triple regimens is well demonstrated. We therefore conclude that these triple regimens did not play any important roles in the patients experiencing an acute coronary syndrome.
 分享
分享




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
