Frank Andersohn, Reinhard Bornemann, Oliver Damm, Martin Frank, Thomas Mittendorf, Ulrike Theidel
{"title":"儿童接种减毒鼻内流感活疫苗——通过卫生技术评估进行分析和评价。","authors":"Frank Andersohn, Reinhard Bornemann, Oliver Damm, Martin Frank, Thomas Mittendorf, Ulrike Theidel","doi":"10.3205/hta000119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Influenza is a worldwide prevalent infectious disease of the respiratory tract annually causing high morbidity and mortality in Germany. Influenza is preventable by vaccination and this vaccination is so far recommended by the The German Standing Committee on Vaccination (STIKO) as a standard vaccination for people from the age of 60 onwards. Up to date a parenterally administered trivalent inactivated vaccine (TIV) has been in use almost exclusively. Since 2011 however a live-attenuated vaccine (LAIV) has been approved additionally. Consecutively, since 2013 the STIKO recommends LAIV (besides TIV) for children from 2 to 17 years of age, within the scope of vaccination by specified indications. LAIV should be preferred administered in children from 2 to 6 of age. The objective of this Health Technology Assessment (HTA) is to address various research issues regarding the vaccination of children with LAIV. The analysis was performed from a medical, epidemiological and health economic perspective, as well as from an ethical, social and legal point of view.</p><p><strong>Method: </strong>An extensive systematic database research was performed to obtain relevant information. In addition a supplementary research by hand was done. Identified literature was screened in two passes by two independent reviewers using predefined inclusion and exclusion criteria. Included literature was evaluated in full-text using acknowledged standards. Studies were graded with the highest level of evidence (1++), if they met the criteria of European Medicines Agency (EMA)-Guidance: Points to consider on applications with 1. meta-analyses; 2. one pivotal study.</p><p><strong>Results: </strong>For the medical section, the age of the study participants ranges from 6 months to 17 years. Regarding study efficacy, in children aged 6 months to ≤7 years, LAIV is superior to placebo as well as to a vac-cination with TIV (Relative Risk Reduction - RRR - of laboratory confirmed influenza infection approx. 80% and 50%, respectively). In children aged >7 to 17 years (= 18th year of their lives), LAIV is superior to a vaccination with TIV (RRR 32%). For this age group, no studies that compared LAIV with placebo were identified. It can be concluded that there is high evidence for superior efficacy of LAIV (compared to placebo or TIV) among children aged 6 months to ≤7 years. For children from >7 to 17 years, there is moderate evidence for superiority of LAIV for children with asthma, while direct evidence for children from the general population is lacking for this age group. Due to the efficacy of LAIV in children aged 6 months to ≤7 years (high evidence) and the efficacy of LAIV in children with asthma aged >7 to 17 years (moderate evidence), LAIV is also very likely to be efficacious among children in the general population aged >7 to 17 years (indirect evidence). In the included studies with children aged 2 to 17 years, LAIV was safe and well-tolerated; while in younger children LAIV may increase the risk of obstruction of the airways (e.g. wheezing). In the majority of the evaluated epidemiological studies, LAIV proved to be effective in the prevention of influenza among children aged 2-17 years under everyday conditions (effectiveness). The trend appears to indicate that LAIV is more effective than TIV, although this can only be based on limited evidence for methodological reasons (observational studies). In addition to a direct protective effect for vaccinated children themselves, indirect protective (\"herd protection\") effects were reported among non-vaccinated elderly population groups, even at relatively low vaccination coverage of children. With regard to safety, LAIV generally can be considered equivalent to TIV. This also applies to the use among children with mild chronically obstructive conditions, from whom LAIV therefore does not have to be withheld. In all included epidemiological studies, there was some risk of bias identified, e.g. due to residual confounding or other methodology-related sources of error. In the evaluated studies, both the vaccination of children with previous illnesses and the routine vaccination of (healthy) children frequently involve cost savings. This is especially the case if one includes indirect costs from a societal perspective. From a payer perspective, a routine vaccination of children is often regarded as a highly cost-effective intervention. However, not all of the studies arrive at consistent results. In isolated cases, relatively high levels of cost-effectiveness are reported that make it difficult to perform a conclusive assessment from an economic perspective. Based on the included studies, it is not possible to make a clear statement about the budget impact of using LAIV. None of the evaluated studies provides results for the context of the German healthcare setting. The efficacy of the vaccine, physicians' recommendations, and a potential reduction in influenza symptoms appear to play a role in the vaccination decision taken by parents/custodians on behalf of their children. Major barriers to the utilization of influenza vaccination services are a low level of perception and an underestimation of the disease risk, reservations concerning the safety and efficacy of the vaccine, and potential side effects of the vaccine. For some of the parents surveyed, the question as to whether the vaccine is administered as an injection or nasal spray might also be important.</p><p><strong>Conclusion: </strong>In children aged 2 to 17 years, the use of LAIV can lead to a reduction of the number of influenza cases and the associated burden of disease. In addition, indirect preventive effects may be expected, especially among elderly age groups. Currently there are no data available for the German healthcare setting. Long-term direct and indirect effectiveness and safety should be supported by surveillance programs with a broader use of LAIV. Since there is no general model available for the German healthcare setting, statements concerning the cost-effectiveness can be made only with precaution. Beside this there is a need to conduct health eco-nomic studies to show the impact of influenza vaccination for children in Germany. Such studies should be based on a dynamic transmission model. Only these models are able to include the indirect protective effects of vaccination correctly. With regard to ethical, social and legal aspects, physicians should discuss with parents the motivations for vaccinating their children and upcoming barriers in order to achieve broader vaccination coverage. The present HTA provides an extensive basis for further scientific approaches and pending decisions relating to health policy.</p>","PeriodicalId":89142,"journal":{"name":"GMS health technology assessment","volume":"10 ","pages":"Doc03"},"PeriodicalIF":0.0000,"publicationDate":"2014-10-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.3205/hta000119","citationCount":"12","resultStr":"{\"title\":\"Vaccination of children with a live-attenuated, intranasal influenza vaccine - analysis and evaluation through a Health Technology Assessment.\",\"authors\":\"Frank Andersohn, Reinhard Bornemann, Oliver Damm, Martin Frank, Thomas Mittendorf, Ulrike Theidel\",\"doi\":\"10.3205/hta000119\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Influenza is a worldwide prevalent infectious disease of the respiratory tract annually causing high morbidity and mortality in Germany. Influenza is preventable by vaccination and this vaccination is so far recommended by the The German Standing Committee on Vaccination (STIKO) as a standard vaccination for people from the age of 60 onwards. Up to date a parenterally administered trivalent inactivated vaccine (TIV) has been in use almost exclusively. Since 2011 however a live-attenuated vaccine (LAIV) has been approved additionally. Consecutively, since 2013 the STIKO recommends LAIV (besides TIV) for children from 2 to 17 years of age, within the scope of vaccination by specified indications. LAIV should be preferred administered in children from 2 to 6 of age. The objective of this Health Technology Assessment (HTA) is to address various research issues regarding the vaccination of children with LAIV. The analysis was performed from a medical, epidemiological and health economic perspective, as well as from an ethical, social and legal point of view.</p><p><strong>Method: </strong>An extensive systematic database research was performed to obtain relevant information. In addition a supplementary research by hand was done. Identified literature was screened in two passes by two independent reviewers using predefined inclusion and exclusion criteria. Included literature was evaluated in full-text using acknowledged standards. Studies were graded with the highest level of evidence (1++), if they met the criteria of European Medicines Agency (EMA)-Guidance: Points to consider on applications with 1. meta-analyses; 2. one pivotal study.</p><p><strong>Results: </strong>For the medical section, the age of the study participants ranges from 6 months to 17 years. Regarding study efficacy, in children aged 6 months to ≤7 years, LAIV is superior to placebo as well as to a vac-cination with TIV (Relative Risk Reduction - RRR - of laboratory confirmed influenza infection approx. 80% and 50%, respectively). In children aged >7 to 17 years (= 18th year of their lives), LAIV is superior to a vaccination with TIV (RRR 32%). For this age group, no studies that compared LAIV with placebo were identified. It can be concluded that there is high evidence for superior efficacy of LAIV (compared to placebo or TIV) among children aged 6 months to ≤7 years. For children from >7 to 17 years, there is moderate evidence for superiority of LAIV for children with asthma, while direct evidence for children from the general population is lacking for this age group. Due to the efficacy of LAIV in children aged 6 months to ≤7 years (high evidence) and the efficacy of LAIV in children with asthma aged >7 to 17 years (moderate evidence), LAIV is also very likely to be efficacious among children in the general population aged >7 to 17 years (indirect evidence). In the included studies with children aged 2 to 17 years, LAIV was safe and well-tolerated; while in younger children LAIV may increase the risk of obstruction of the airways (e.g. wheezing). In the majority of the evaluated epidemiological studies, LAIV proved to be effective in the prevention of influenza among children aged 2-17 years under everyday conditions (effectiveness). The trend appears to indicate that LAIV is more effective than TIV, although this can only be based on limited evidence for methodological reasons (observational studies). In addition to a direct protective effect for vaccinated children themselves, indirect protective (\\\"herd protection\\\") effects were reported among non-vaccinated elderly population groups, even at relatively low vaccination coverage of children. With regard to safety, LAIV generally can be considered equivalent to TIV. This also applies to the use among children with mild chronically obstructive conditions, from whom LAIV therefore does not have to be withheld. In all included epidemiological studies, there was some risk of bias identified, e.g. due to residual confounding or other methodology-related sources of error. In the evaluated studies, both the vaccination of children with previous illnesses and the routine vaccination of (healthy) children frequently involve cost savings. This is especially the case if one includes indirect costs from a societal perspective. From a payer perspective, a routine vaccination of children is often regarded as a highly cost-effective intervention. However, not all of the studies arrive at consistent results. In isolated cases, relatively high levels of cost-effectiveness are reported that make it difficult to perform a conclusive assessment from an economic perspective. Based on the included studies, it is not possible to make a clear statement about the budget impact of using LAIV. None of the evaluated studies provides results for the context of the German healthcare setting. The efficacy of the vaccine, physicians' recommendations, and a potential reduction in influenza symptoms appear to play a role in the vaccination decision taken by parents/custodians on behalf of their children. Major barriers to the utilization of influenza vaccination services are a low level of perception and an underestimation of the disease risk, reservations concerning the safety and efficacy of the vaccine, and potential side effects of the vaccine. For some of the parents surveyed, the question as to whether the vaccine is administered as an injection or nasal spray might also be important.</p><p><strong>Conclusion: </strong>In children aged 2 to 17 years, the use of LAIV can lead to a reduction of the number of influenza cases and the associated burden of disease. In addition, indirect preventive effects may be expected, especially among elderly age groups. Currently there are no data available for the German healthcare setting. Long-term direct and indirect effectiveness and safety should be supported by surveillance programs with a broader use of LAIV. Since there is no general model available for the German healthcare setting, statements concerning the cost-effectiveness can be made only with precaution. Beside this there is a need to conduct health eco-nomic studies to show the impact of influenza vaccination for children in Germany. Such studies should be based on a dynamic transmission model. Only these models are able to include the indirect protective effects of vaccination correctly. With regard to ethical, social and legal aspects, physicians should discuss with parents the motivations for vaccinating their children and upcoming barriers in order to achieve broader vaccination coverage. The present HTA provides an extensive basis for further scientific approaches and pending decisions relating to health policy.</p>\",\"PeriodicalId\":89142,\"journal\":{\"name\":\"GMS health technology assessment\",\"volume\":\"10 \",\"pages\":\"Doc03\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-10-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.3205/hta000119\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GMS health technology assessment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3205/hta000119\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS health technology assessment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/hta000119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Vaccination of children with a live-attenuated, intranasal influenza vaccine - analysis and evaluation through a Health Technology Assessment.
Background: Influenza is a worldwide prevalent infectious disease of the respiratory tract annually causing high morbidity and mortality in Germany. Influenza is preventable by vaccination and this vaccination is so far recommended by the The German Standing Committee on Vaccination (STIKO) as a standard vaccination for people from the age of 60 onwards. Up to date a parenterally administered trivalent inactivated vaccine (TIV) has been in use almost exclusively. Since 2011 however a live-attenuated vaccine (LAIV) has been approved additionally. Consecutively, since 2013 the STIKO recommends LAIV (besides TIV) for children from 2 to 17 years of age, within the scope of vaccination by specified indications. LAIV should be preferred administered in children from 2 to 6 of age. The objective of this Health Technology Assessment (HTA) is to address various research issues regarding the vaccination of children with LAIV. The analysis was performed from a medical, epidemiological and health economic perspective, as well as from an ethical, social and legal point of view.
Method: An extensive systematic database research was performed to obtain relevant information. In addition a supplementary research by hand was done. Identified literature was screened in two passes by two independent reviewers using predefined inclusion and exclusion criteria. Included literature was evaluated in full-text using acknowledged standards. Studies were graded with the highest level of evidence (1++), if they met the criteria of European Medicines Agency (EMA)-Guidance: Points to consider on applications with 1. meta-analyses; 2. one pivotal study.
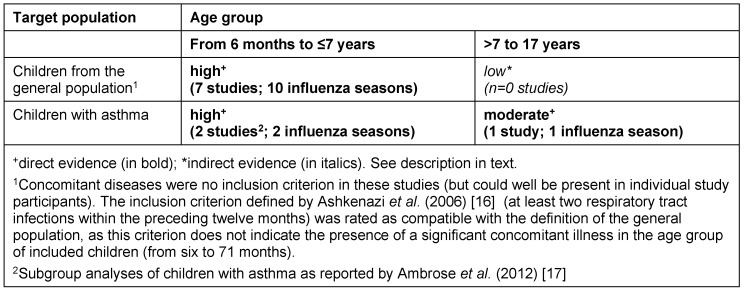
Results: For the medical section, the age of the study participants ranges from 6 months to 17 years. Regarding study efficacy, in children aged 6 months to ≤7 years, LAIV is superior to placebo as well as to a vac-cination with TIV (Relative Risk Reduction - RRR - of laboratory confirmed influenza infection approx. 80% and 50%, respectively). In children aged >7 to 17 years (= 18th year of their lives), LAIV is superior to a vaccination with TIV (RRR 32%). For this age group, no studies that compared LAIV with placebo were identified. It can be concluded that there is high evidence for superior efficacy of LAIV (compared to placebo or TIV) among children aged 6 months to ≤7 years. For children from >7 to 17 years, there is moderate evidence for superiority of LAIV for children with asthma, while direct evidence for children from the general population is lacking for this age group. Due to the efficacy of LAIV in children aged 6 months to ≤7 years (high evidence) and the efficacy of LAIV in children with asthma aged >7 to 17 years (moderate evidence), LAIV is also very likely to be efficacious among children in the general population aged >7 to 17 years (indirect evidence). In the included studies with children aged 2 to 17 years, LAIV was safe and well-tolerated; while in younger children LAIV may increase the risk of obstruction of the airways (e.g. wheezing). In the majority of the evaluated epidemiological studies, LAIV proved to be effective in the prevention of influenza among children aged 2-17 years under everyday conditions (effectiveness). The trend appears to indicate that LAIV is more effective than TIV, although this can only be based on limited evidence for methodological reasons (observational studies). In addition to a direct protective effect for vaccinated children themselves, indirect protective ("herd protection") effects were reported among non-vaccinated elderly population groups, even at relatively low vaccination coverage of children. With regard to safety, LAIV generally can be considered equivalent to TIV. This also applies to the use among children with mild chronically obstructive conditions, from whom LAIV therefore does not have to be withheld. In all included epidemiological studies, there was some risk of bias identified, e.g. due to residual confounding or other methodology-related sources of error. In the evaluated studies, both the vaccination of children with previous illnesses and the routine vaccination of (healthy) children frequently involve cost savings. This is especially the case if one includes indirect costs from a societal perspective. From a payer perspective, a routine vaccination of children is often regarded as a highly cost-effective intervention. However, not all of the studies arrive at consistent results. In isolated cases, relatively high levels of cost-effectiveness are reported that make it difficult to perform a conclusive assessment from an economic perspective. Based on the included studies, it is not possible to make a clear statement about the budget impact of using LAIV. None of the evaluated studies provides results for the context of the German healthcare setting. The efficacy of the vaccine, physicians' recommendations, and a potential reduction in influenza symptoms appear to play a role in the vaccination decision taken by parents/custodians on behalf of their children. Major barriers to the utilization of influenza vaccination services are a low level of perception and an underestimation of the disease risk, reservations concerning the safety and efficacy of the vaccine, and potential side effects of the vaccine. For some of the parents surveyed, the question as to whether the vaccine is administered as an injection or nasal spray might also be important.
Conclusion: In children aged 2 to 17 years, the use of LAIV can lead to a reduction of the number of influenza cases and the associated burden of disease. In addition, indirect preventive effects may be expected, especially among elderly age groups. Currently there are no data available for the German healthcare setting. Long-term direct and indirect effectiveness and safety should be supported by surveillance programs with a broader use of LAIV. Since there is no general model available for the German healthcare setting, statements concerning the cost-effectiveness can be made only with precaution. Beside this there is a need to conduct health eco-nomic studies to show the impact of influenza vaccination for children in Germany. Such studies should be based on a dynamic transmission model. Only these models are able to include the indirect protective effects of vaccination correctly. With regard to ethical, social and legal aspects, physicians should discuss with parents the motivations for vaccinating their children and upcoming barriers in order to achieve broader vaccination coverage. The present HTA provides an extensive basis for further scientific approaches and pending decisions relating to health policy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
