Mojib Fallah, Sönke Detlefsen, Alan P Ainsworth, Claus W Fristrup, Michael B Mortensen, Per Pfeiffer, Line S Tarpgaard, Martin Graversen
{"title":"反复加压腹腔喷雾化疗(PIPAC)治疗腹膜转移的活检部位选择对腹膜回归分级评分(PRGS)的重要性。","authors":"Mojib Fallah, Sönke Detlefsen, Alan P Ainsworth, Claus W Fristrup, Michael B Mortensen, Per Pfeiffer, Line S Tarpgaard, Martin Graversen","doi":"10.1515/pp-2022-0108","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The four-tiered peritoneal regression grading score (PRGS) is used for histological response evaluation in patients with peritoneal metastasis (PM) treated with pressurized intraperitoneal aerosol chemotherapy (PIPAC). Four quadrant biopsies (QBs) from the parietal peritoneum should be assessed by PRGS, but consensus on biopsy site strategy for follow-up biopsies during repeated PIPACs is lacking. We aimed to evaluate whether there is a difference between PRGS in QBs from clips marked PM (QB-CM) compared to biopsies from PM with the visually most malignant features (worst biopsy, WB).</p><p><strong>Methods: </strong>Prospective, descriptive study. During the first PIPAC, index QBs sites were marked with metal clips. During the second PIPAC, an independent surgical oncologist selected biopsy site for WB and biopsies were taken from QB-CM and WB. One blinded pathologist evaluated all biopsies according to PRGS. From each biopsy, three step sections were stained H&E, followed by an immunostained section, and another three step sections stained H&E.</p><p><strong>Results: </strong>Thirty-four patients were included from March 2020 to May 2021. Median age 64 years. Maximum mean PRGS in QB-CM at PIPAC 1 was 3.3 (SD 1.2). Maximum mean PRGS in QB-CM at PIPAC 2 was 2.6 (SD 1.2), whereas mean PRGS in WB at PIPAC 2 was 2.4 (SD 1.3). At PIPAC 2, there was agreement between maximum PRGS from QB-CM and PRGS from WB in 21 patients. Maximum PRGS from QB-CM was higher in nine and lower in four patients, compared to PRGS from WB.</p><p><strong>Conclusions: </strong>Biopsies from QB-CM did not overestimate treatment response compared to biopsies from WB.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"7 3","pages":"143-148"},"PeriodicalIF":2.4000,"publicationDate":"2022-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9467898/pdf/","citationCount":"2","resultStr":"{\"title\":\"Importance of biopsy site selection for peritoneal regression grading score (PRGS) in peritoneal metastasis treated with repeated pressurized intraperitoneal aerosol chemotherapy (PIPAC).\",\"authors\":\"Mojib Fallah, Sönke Detlefsen, Alan P Ainsworth, Claus W Fristrup, Michael B Mortensen, Per Pfeiffer, Line S Tarpgaard, Martin Graversen\",\"doi\":\"10.1515/pp-2022-0108\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The four-tiered peritoneal regression grading score (PRGS) is used for histological response evaluation in patients with peritoneal metastasis (PM) treated with pressurized intraperitoneal aerosol chemotherapy (PIPAC). Four quadrant biopsies (QBs) from the parietal peritoneum should be assessed by PRGS, but consensus on biopsy site strategy for follow-up biopsies during repeated PIPACs is lacking. We aimed to evaluate whether there is a difference between PRGS in QBs from clips marked PM (QB-CM) compared to biopsies from PM with the visually most malignant features (worst biopsy, WB).</p><p><strong>Methods: </strong>Prospective, descriptive study. During the first PIPAC, index QBs sites were marked with metal clips. During the second PIPAC, an independent surgical oncologist selected biopsy site for WB and biopsies were taken from QB-CM and WB. One blinded pathologist evaluated all biopsies according to PRGS. From each biopsy, three step sections were stained H&E, followed by an immunostained section, and another three step sections stained H&E.</p><p><strong>Results: </strong>Thirty-four patients were included from March 2020 to May 2021. Median age 64 years. Maximum mean PRGS in QB-CM at PIPAC 1 was 3.3 (SD 1.2). Maximum mean PRGS in QB-CM at PIPAC 2 was 2.6 (SD 1.2), whereas mean PRGS in WB at PIPAC 2 was 2.4 (SD 1.3). At PIPAC 2, there was agreement between maximum PRGS from QB-CM and PRGS from WB in 21 patients. Maximum PRGS from QB-CM was higher in nine and lower in four patients, compared to PRGS from WB.</p><p><strong>Conclusions: </strong>Biopsies from QB-CM did not overestimate treatment response compared to biopsies from WB.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"7 3\",\"pages\":\"143-148\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2022-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9467898/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2022-0108\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2022-0108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Importance of biopsy site selection for peritoneal regression grading score (PRGS) in peritoneal metastasis treated with repeated pressurized intraperitoneal aerosol chemotherapy (PIPAC).
Objectives: The four-tiered peritoneal regression grading score (PRGS) is used for histological response evaluation in patients with peritoneal metastasis (PM) treated with pressurized intraperitoneal aerosol chemotherapy (PIPAC). Four quadrant biopsies (QBs) from the parietal peritoneum should be assessed by PRGS, but consensus on biopsy site strategy for follow-up biopsies during repeated PIPACs is lacking. We aimed to evaluate whether there is a difference between PRGS in QBs from clips marked PM (QB-CM) compared to biopsies from PM with the visually most malignant features (worst biopsy, WB).
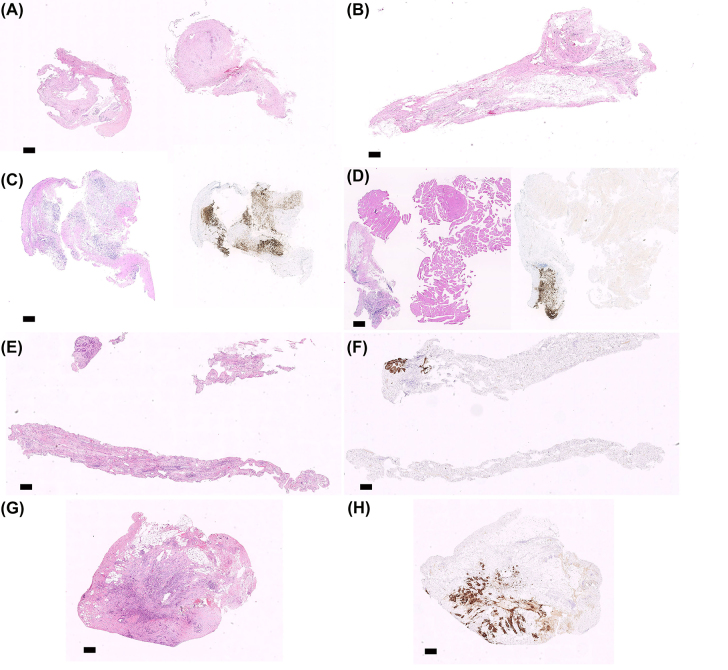
Methods: Prospective, descriptive study. During the first PIPAC, index QBs sites were marked with metal clips. During the second PIPAC, an independent surgical oncologist selected biopsy site for WB and biopsies were taken from QB-CM and WB. One blinded pathologist evaluated all biopsies according to PRGS. From each biopsy, three step sections were stained H&E, followed by an immunostained section, and another three step sections stained H&E.
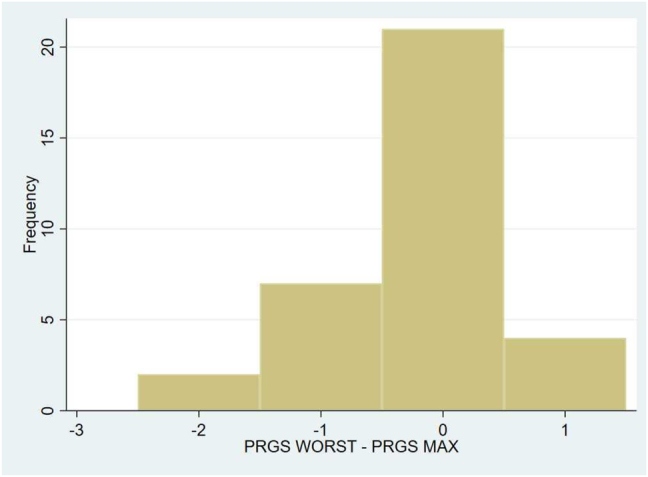
Results: Thirty-four patients were included from March 2020 to May 2021. Median age 64 years. Maximum mean PRGS in QB-CM at PIPAC 1 was 3.3 (SD 1.2). Maximum mean PRGS in QB-CM at PIPAC 2 was 2.6 (SD 1.2), whereas mean PRGS in WB at PIPAC 2 was 2.4 (SD 1.3). At PIPAC 2, there was agreement between maximum PRGS from QB-CM and PRGS from WB in 21 patients. Maximum PRGS from QB-CM was higher in nine and lower in four patients, compared to PRGS from WB.
Conclusions: Biopsies from QB-CM did not overestimate treatment response compared to biopsies from WB.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
