Abdulhadi Jfri, Bonnie Leung, Jordan T Said, Yevgeniy Semenov, Nicole R LeBoeuf
{"title":"免疫检查点抑制剂对银屑病逆亚型患病率的影响","authors":"Abdulhadi Jfri, Bonnie Leung, Jordan T Said, Yevgeniy Semenov, Nicole R LeBoeuf","doi":"10.1093/immadv/ltac016","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cutaneous immune-related adverse events (irAEs) are the most common irAEs caused by immune-checkpoint inhibitors (ICI). Psoriasiform eruptions, both <i>de novo</i> and flares, may occur. Evidence is lacking on inverse psoriasis subtype.</p><p><strong>Methods: </strong>A retrospective study was conducted at Dana-Farber Cancer Institute/Mass General Brigham through February 2020 using databases. Confirmed inverse psoriasis cases pre-/post-ICI initiation either independently or in conjunction with other psoriasis subtypes were included. Known psoriasis cases without flare post-ICI were excluded.</p><p><strong>Results: </strong>A total of 262 (3%) individuals with any ICI-mediated psoriasiform cutaneous irAE were identified out of the 8683 DFCI ICI-treated patients. Of these, 13 (5% of psoriasis patients) had inverse psoriasis (mean age 68.7 years; 7/13 male sex). Median (range) time from ICI initiation to inverse psoriasis development or flare was 7 (4-12) and 3.5 (2-6) weeks, respectively. Pruritus occurred in 12/13 (92.30%) cases. 11 (85%) had inguinal involvement; other sites included gluteal cleft (6; 46%), inframammary (3; 23%), perianal (2; 15%), axilla (2; 15%), umbilicus (2; 15%), and infra-abdominal folds (1; 8%). Most (9/13) individuals had more than one site involved. The Common Terminology Criteria for Adverse Events severity was 1 in 10 (76.92%) individuals and 2 in 3 (15.38%) individuals. Six (46.15%) patients were treated initially by oncology with topical (nystatin, econazole, or clotrimazole) or systemic antifungals (fluconazole) for median (range) of 3.5 (1-7) months without improvement, for presumed candida intertrigo.</p><p><strong>Conclusion: </strong>Patients on ICI may develop inverse psoriasis, which may be initially confused for fungal intertrigo. Delayed diagnosis can prolong symptoms, while patients are treated ineffectively with topical/systemic antifungals for presumed candida infection. Oncologist and dermatologist awareness is important to improve diagnosis of ICI-mediated inverse psoriasis, its management and affected patients' quality of life.</p>","PeriodicalId":73353,"journal":{"name":"Immunotherapy advances","volume":null,"pages":null},"PeriodicalIF":4.1000,"publicationDate":"2022-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/60/68/ltac016.PMC9525015.pdf","citationCount":"3","resultStr":"{\"title\":\"Prevalence of inverse psoriasis subtype with immune checkpoint inhibitors.\",\"authors\":\"Abdulhadi Jfri, Bonnie Leung, Jordan T Said, Yevgeniy Semenov, Nicole R LeBoeuf\",\"doi\":\"10.1093/immadv/ltac016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cutaneous immune-related adverse events (irAEs) are the most common irAEs caused by immune-checkpoint inhibitors (ICI). Psoriasiform eruptions, both <i>de novo</i> and flares, may occur. Evidence is lacking on inverse psoriasis subtype.</p><p><strong>Methods: </strong>A retrospective study was conducted at Dana-Farber Cancer Institute/Mass General Brigham through February 2020 using databases. Confirmed inverse psoriasis cases pre-/post-ICI initiation either independently or in conjunction with other psoriasis subtypes were included. Known psoriasis cases without flare post-ICI were excluded.</p><p><strong>Results: </strong>A total of 262 (3%) individuals with any ICI-mediated psoriasiform cutaneous irAE were identified out of the 8683 DFCI ICI-treated patients. Of these, 13 (5% of psoriasis patients) had inverse psoriasis (mean age 68.7 years; 7/13 male sex). Median (range) time from ICI initiation to inverse psoriasis development or flare was 7 (4-12) and 3.5 (2-6) weeks, respectively. Pruritus occurred in 12/13 (92.30%) cases. 11 (85%) had inguinal involvement; other sites included gluteal cleft (6; 46%), inframammary (3; 23%), perianal (2; 15%), axilla (2; 15%), umbilicus (2; 15%), and infra-abdominal folds (1; 8%). Most (9/13) individuals had more than one site involved. The Common Terminology Criteria for Adverse Events severity was 1 in 10 (76.92%) individuals and 2 in 3 (15.38%) individuals. Six (46.15%) patients were treated initially by oncology with topical (nystatin, econazole, or clotrimazole) or systemic antifungals (fluconazole) for median (range) of 3.5 (1-7) months without improvement, for presumed candida intertrigo.</p><p><strong>Conclusion: </strong>Patients on ICI may develop inverse psoriasis, which may be initially confused for fungal intertrigo. Delayed diagnosis can prolong symptoms, while patients are treated ineffectively with topical/systemic antifungals for presumed candida infection. Oncologist and dermatologist awareness is important to improve diagnosis of ICI-mediated inverse psoriasis, its management and affected patients' quality of life.</p>\",\"PeriodicalId\":73353,\"journal\":{\"name\":\"Immunotherapy advances\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2022-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/60/68/ltac016.PMC9525015.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Immunotherapy advances\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/immadv/ltac016\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunotherapy advances","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/immadv/ltac016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Prevalence of inverse psoriasis subtype with immune checkpoint inhibitors.
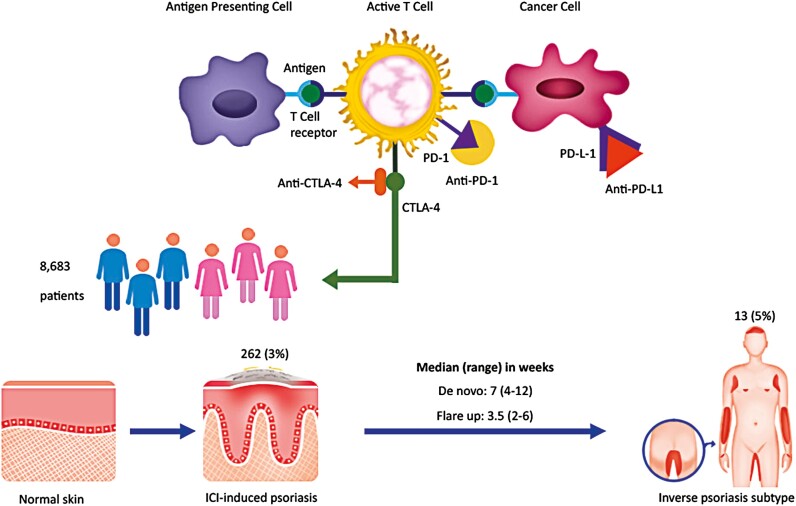
Background: Cutaneous immune-related adverse events (irAEs) are the most common irAEs caused by immune-checkpoint inhibitors (ICI). Psoriasiform eruptions, both de novo and flares, may occur. Evidence is lacking on inverse psoriasis subtype.
Methods: A retrospective study was conducted at Dana-Farber Cancer Institute/Mass General Brigham through February 2020 using databases. Confirmed inverse psoriasis cases pre-/post-ICI initiation either independently or in conjunction with other psoriasis subtypes were included. Known psoriasis cases without flare post-ICI were excluded.
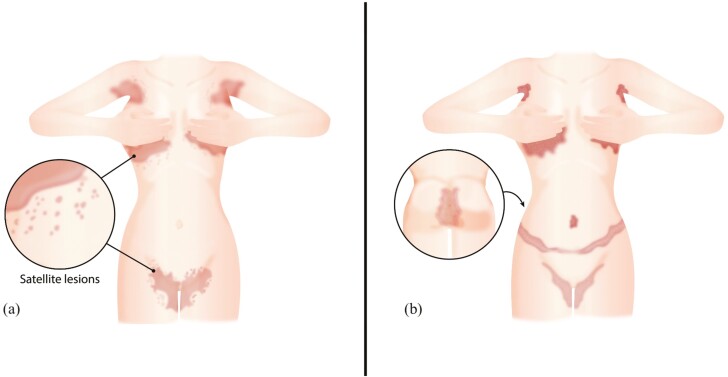
Results: A total of 262 (3%) individuals with any ICI-mediated psoriasiform cutaneous irAE were identified out of the 8683 DFCI ICI-treated patients. Of these, 13 (5% of psoriasis patients) had inverse psoriasis (mean age 68.7 years; 7/13 male sex). Median (range) time from ICI initiation to inverse psoriasis development or flare was 7 (4-12) and 3.5 (2-6) weeks, respectively. Pruritus occurred in 12/13 (92.30%) cases. 11 (85%) had inguinal involvement; other sites included gluteal cleft (6; 46%), inframammary (3; 23%), perianal (2; 15%), axilla (2; 15%), umbilicus (2; 15%), and infra-abdominal folds (1; 8%). Most (9/13) individuals had more than one site involved. The Common Terminology Criteria for Adverse Events severity was 1 in 10 (76.92%) individuals and 2 in 3 (15.38%) individuals. Six (46.15%) patients were treated initially by oncology with topical (nystatin, econazole, or clotrimazole) or systemic antifungals (fluconazole) for median (range) of 3.5 (1-7) months without improvement, for presumed candida intertrigo.
Conclusion: Patients on ICI may develop inverse psoriasis, which may be initially confused for fungal intertrigo. Delayed diagnosis can prolong symptoms, while patients are treated ineffectively with topical/systemic antifungals for presumed candida infection. Oncologist and dermatologist awareness is important to improve diagnosis of ICI-mediated inverse psoriasis, its management and affected patients' quality of life.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
