Shanal Kumar , Michael Pallin , Georgia Soldatos , Helena Teede
{"title":"连续血糖监测与参考标准口服糖耐量试验检测囊性纤维化患者血糖异常的比较:系统综述","authors":"Shanal Kumar , Michael Pallin , Georgia Soldatos , Helena Teede","doi":"10.1016/j.jcte.2022.100305","DOIUrl":null,"url":null,"abstract":"<div><h3>Aims</h3><p>Increasing evidence for benefit of early detection of cystic fibrosis related diabetes (CFRD) coupled with limitations of current diagnostic investigations has led to interest and utilisation of continuous glucose monitoring (CGM). We conducted a systematic review to assess current evidence on CGM compared to reference standard oral glucose tolerance test for the detection of dysglycemia in people with cystic fibrosis without confirmed diabetes.</p></div><div><h3>Methods</h3><p>MEDLINE, Embase, CENTRAL, Evidence-Based Medicine Reviews, grey literature and six relevant journals were searched for studies published after year 2000. Studies reporting contemporaneous CGM metrics and oral glucose tolerance test results were included. Outcomes on oral glucose tolerance tests were categorised into a) normal, b) abnormal (indeterminate and impaired) or c) diabetic as defined by American Diabetes Association criteria. CGM outcomes were defined as hyperglycemia (≥1 peak sensor glucose ≥ 200 mg/dL), dysglycemia (≥1 peak sensor glucose ≥ 140–199 mg/dL) or normoglycemia (all sensor glucose peaks < 140 mg/dL). CGM hyperglycemia in people with normal or abnormal glucose tolerances was used to define an arbitrary CGM-diagnosis of diabetes. The Quality Assessment of Diagnostic Accuracy Studies tool was used to assess risk of bias. Primary outcome was relative risk of an arbitrary CGM-diagnosis of diabetes compared to the oral glucose tolerance test.</p></div><div><h3>Results</h3><p>We identified 1277 publications, of which 19 studies were eligible comprising total of 416 individuals with contemporaneous CGM and oral glucose tolerance test results. Relative risk of an arbitrary CGM-diagnosis of diabetes compared to oral glucose tolerance test was 2.92. Studies analysed were highly heterogenous, prone to bias and inadequately assessed longitudinal associations between CGM and relevant disease-specific sequela.</p></div><div><h3>Conclusions</h3><p>A single reading > 200 mg/dL on CGM is not appropriate for the diagnosis of CFRD. Prospective studies correlating CGM metrics to disease-specific outcomes are needed to determine appropriate cut-points.</p></div>","PeriodicalId":46328,"journal":{"name":"Journal of Clinical and Translational Endocrinology","volume":"30 ","pages":"Article 100305"},"PeriodicalIF":3.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b7/a9/main.PMC9529501.pdf","citationCount":"2","resultStr":"{\"title\":\"Comparison of continuous glucose monitoring to reference standard oral glucose tolerance test for the detection of dysglycemia in cystic Fibrosis: A systematic review\",\"authors\":\"Shanal Kumar , Michael Pallin , Georgia Soldatos , Helena Teede\",\"doi\":\"10.1016/j.jcte.2022.100305\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Aims</h3><p>Increasing evidence for benefit of early detection of cystic fibrosis related diabetes (CFRD) coupled with limitations of current diagnostic investigations has led to interest and utilisation of continuous glucose monitoring (CGM). We conducted a systematic review to assess current evidence on CGM compared to reference standard oral glucose tolerance test for the detection of dysglycemia in people with cystic fibrosis without confirmed diabetes.</p></div><div><h3>Methods</h3><p>MEDLINE, Embase, CENTRAL, Evidence-Based Medicine Reviews, grey literature and six relevant journals were searched for studies published after year 2000. Studies reporting contemporaneous CGM metrics and oral glucose tolerance test results were included. Outcomes on oral glucose tolerance tests were categorised into a) normal, b) abnormal (indeterminate and impaired) or c) diabetic as defined by American Diabetes Association criteria. CGM outcomes were defined as hyperglycemia (≥1 peak sensor glucose ≥ 200 mg/dL), dysglycemia (≥1 peak sensor glucose ≥ 140–199 mg/dL) or normoglycemia (all sensor glucose peaks < 140 mg/dL). CGM hyperglycemia in people with normal or abnormal glucose tolerances was used to define an arbitrary CGM-diagnosis of diabetes. The Quality Assessment of Diagnostic Accuracy Studies tool was used to assess risk of bias. Primary outcome was relative risk of an arbitrary CGM-diagnosis of diabetes compared to the oral glucose tolerance test.</p></div><div><h3>Results</h3><p>We identified 1277 publications, of which 19 studies were eligible comprising total of 416 individuals with contemporaneous CGM and oral glucose tolerance test results. Relative risk of an arbitrary CGM-diagnosis of diabetes compared to oral glucose tolerance test was 2.92. Studies analysed were highly heterogenous, prone to bias and inadequately assessed longitudinal associations between CGM and relevant disease-specific sequela.</p></div><div><h3>Conclusions</h3><p>A single reading > 200 mg/dL on CGM is not appropriate for the diagnosis of CFRD. Prospective studies correlating CGM metrics to disease-specific outcomes are needed to determine appropriate cut-points.</p></div>\",\"PeriodicalId\":46328,\"journal\":{\"name\":\"Journal of Clinical and Translational Endocrinology\",\"volume\":\"30 \",\"pages\":\"Article 100305\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b7/a9/main.PMC9529501.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical and Translational Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2214623722000138\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/9/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214623722000138","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Comparison of continuous glucose monitoring to reference standard oral glucose tolerance test for the detection of dysglycemia in cystic Fibrosis: A systematic review
Aims
Increasing evidence for benefit of early detection of cystic fibrosis related diabetes (CFRD) coupled with limitations of current diagnostic investigations has led to interest and utilisation of continuous glucose monitoring (CGM). We conducted a systematic review to assess current evidence on CGM compared to reference standard oral glucose tolerance test for the detection of dysglycemia in people with cystic fibrosis without confirmed diabetes.
Methods
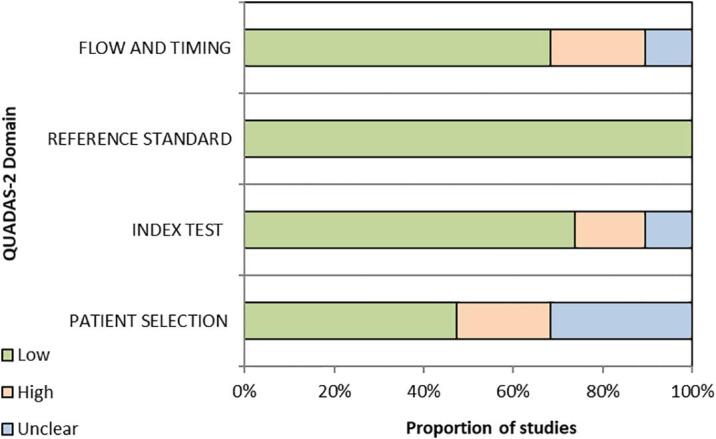
MEDLINE, Embase, CENTRAL, Evidence-Based Medicine Reviews, grey literature and six relevant journals were searched for studies published after year 2000. Studies reporting contemporaneous CGM metrics and oral glucose tolerance test results were included. Outcomes on oral glucose tolerance tests were categorised into a) normal, b) abnormal (indeterminate and impaired) or c) diabetic as defined by American Diabetes Association criteria. CGM outcomes were defined as hyperglycemia (≥1 peak sensor glucose ≥ 200 mg/dL), dysglycemia (≥1 peak sensor glucose ≥ 140–199 mg/dL) or normoglycemia (all sensor glucose peaks < 140 mg/dL). CGM hyperglycemia in people with normal or abnormal glucose tolerances was used to define an arbitrary CGM-diagnosis of diabetes. The Quality Assessment of Diagnostic Accuracy Studies tool was used to assess risk of bias. Primary outcome was relative risk of an arbitrary CGM-diagnosis of diabetes compared to the oral glucose tolerance test.
Results
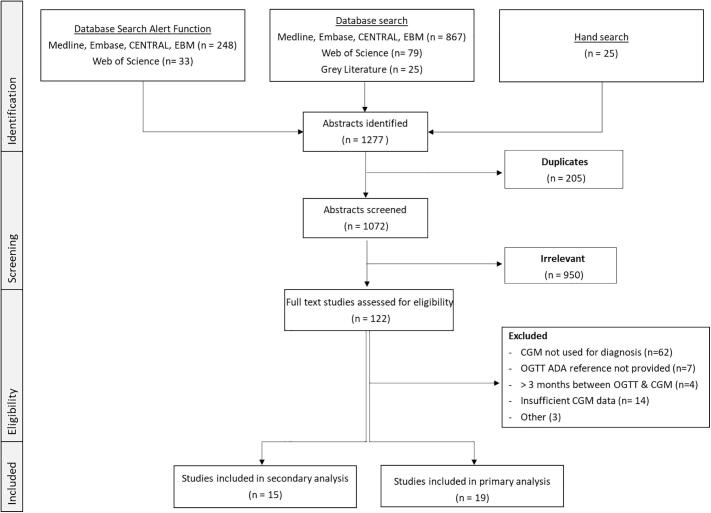
We identified 1277 publications, of which 19 studies were eligible comprising total of 416 individuals with contemporaneous CGM and oral glucose tolerance test results. Relative risk of an arbitrary CGM-diagnosis of diabetes compared to oral glucose tolerance test was 2.92. Studies analysed were highly heterogenous, prone to bias and inadequately assessed longitudinal associations between CGM and relevant disease-specific sequela.
Conclusions
A single reading > 200 mg/dL on CGM is not appropriate for the diagnosis of CFRD. Prospective studies correlating CGM metrics to disease-specific outcomes are needed to determine appropriate cut-points.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
