{"title":"下消化道手术后,彭罗斯引流管的腔内移位表现为便血。","authors":"Roza Mourelatou, Christos Liatsos, Angeliki Bistaraki, Efstathios Nikou","doi":"10.1055/s-0042-1757603","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Although surgical drains are widely used after lower gastrointestinal (GI) procedures, complications may occur. Specifically, sporadic cases of drain migration into a hollow viscus, most commonly regarding active drains and treated with surgical removal, have been reported. Herein, we present a case of a passive drain (penrose) migration into the colon, after segmental sigmoidectomy with primary anastomosis, presented with hematochezia. <b>Methods</b> A 37-year-old male patient suffering from colovesical fistula, due to sigmoid diverticulitis, underwent resection of the fistula, the involved sigmoid segment and the bladder opening, followed by primary anastomosis of the colon and primary closure of the bladder. A penrose catheter was positioned near the anastomosis. <b>Results</b> On 8th postoperative day (POD) the patient had three episodes of hematochezia and blood in the drain collection bag, followed by relative improvement. On 15th POD gas was observed on the drain's collection bag and a new episode of hematochezia led him to sigmoidoscopy. The endoscopy revealed the presence of the penrose drain intraluminally, protruding via an ulcer at the level of the anastomosis. The penrose repositioned outside the lumen and metallic clips were used to approximate the defect. The patient was then fully recovered, discharged, and the drain removed on follow-up. <b>Conclusion</b> To our knowledge this is the first report of drain migration presented with hematochezia, after lower GI surgery, avoided reoperation, and resolved with removal of the drain under direct endoscopic vision.</p>","PeriodicalId":44614,"journal":{"name":"Surgery Journal","volume":" ","pages":"e279-e282"},"PeriodicalIF":0.8000,"publicationDate":"2022-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9550314/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intraluminal Migration of a Penrose Drain Presented with Hematochezia, after Lower Gastrointestinal Surgery.\",\"authors\":\"Roza Mourelatou, Christos Liatsos, Angeliki Bistaraki, Efstathios Nikou\",\"doi\":\"10.1055/s-0042-1757603\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background</b> Although surgical drains are widely used after lower gastrointestinal (GI) procedures, complications may occur. Specifically, sporadic cases of drain migration into a hollow viscus, most commonly regarding active drains and treated with surgical removal, have been reported. Herein, we present a case of a passive drain (penrose) migration into the colon, after segmental sigmoidectomy with primary anastomosis, presented with hematochezia. <b>Methods</b> A 37-year-old male patient suffering from colovesical fistula, due to sigmoid diverticulitis, underwent resection of the fistula, the involved sigmoid segment and the bladder opening, followed by primary anastomosis of the colon and primary closure of the bladder. A penrose catheter was positioned near the anastomosis. <b>Results</b> On 8th postoperative day (POD) the patient had three episodes of hematochezia and blood in the drain collection bag, followed by relative improvement. On 15th POD gas was observed on the drain's collection bag and a new episode of hematochezia led him to sigmoidoscopy. The endoscopy revealed the presence of the penrose drain intraluminally, protruding via an ulcer at the level of the anastomosis. The penrose repositioned outside the lumen and metallic clips were used to approximate the defect. The patient was then fully recovered, discharged, and the drain removed on follow-up. <b>Conclusion</b> To our knowledge this is the first report of drain migration presented with hematochezia, after lower GI surgery, avoided reoperation, and resolved with removal of the drain under direct endoscopic vision.</p>\",\"PeriodicalId\":44614,\"journal\":{\"name\":\"Surgery Journal\",\"volume\":\" \",\"pages\":\"e279-e282\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9550314/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgery Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0042-1757603\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1757603","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Intraluminal Migration of a Penrose Drain Presented with Hematochezia, after Lower Gastrointestinal Surgery.
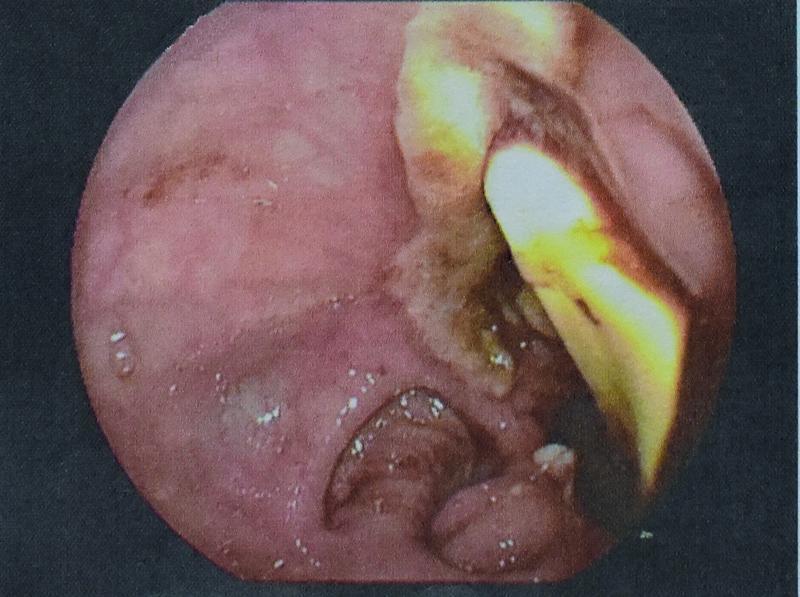
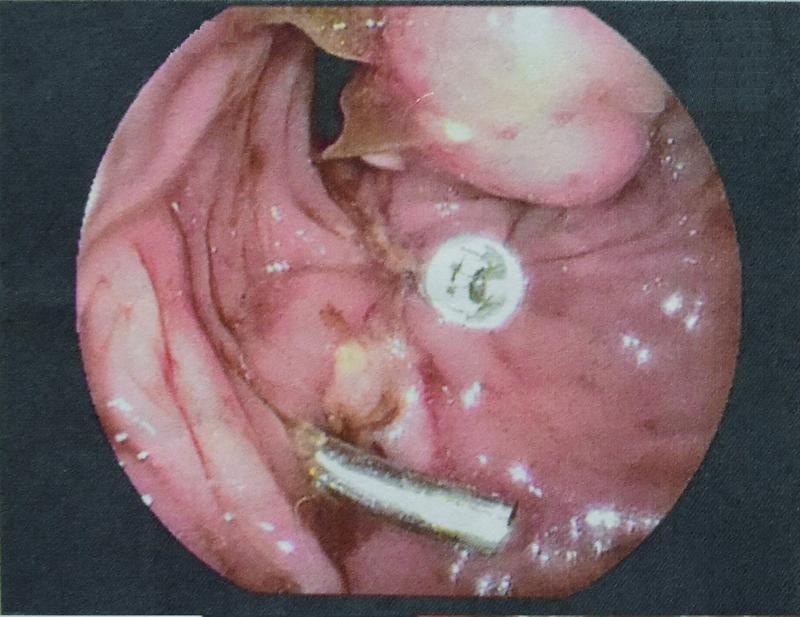
Background Although surgical drains are widely used after lower gastrointestinal (GI) procedures, complications may occur. Specifically, sporadic cases of drain migration into a hollow viscus, most commonly regarding active drains and treated with surgical removal, have been reported. Herein, we present a case of a passive drain (penrose) migration into the colon, after segmental sigmoidectomy with primary anastomosis, presented with hematochezia. Methods A 37-year-old male patient suffering from colovesical fistula, due to sigmoid diverticulitis, underwent resection of the fistula, the involved sigmoid segment and the bladder opening, followed by primary anastomosis of the colon and primary closure of the bladder. A penrose catheter was positioned near the anastomosis. Results On 8th postoperative day (POD) the patient had three episodes of hematochezia and blood in the drain collection bag, followed by relative improvement. On 15th POD gas was observed on the drain's collection bag and a new episode of hematochezia led him to sigmoidoscopy. The endoscopy revealed the presence of the penrose drain intraluminally, protruding via an ulcer at the level of the anastomosis. The penrose repositioned outside the lumen and metallic clips were used to approximate the defect. The patient was then fully recovered, discharged, and the drain removed on follow-up. Conclusion To our knowledge this is the first report of drain migration presented with hematochezia, after lower GI surgery, avoided reoperation, and resolved with removal of the drain under direct endoscopic vision.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
