Sang-Jae Lee, Wooil Kwon, Mee Joo Kang, Jin-Young Jang, Ye Rim Chang, Woohyun Jung, Sun-Whe Kim
{"title":"局部晚期肝外胆管癌的临床特点及生存结局。","authors":"Sang-Jae Lee, Wooil Kwon, Mee Joo Kang, Jin-Young Jang, Ye Rim Chang, Woohyun Jung, Sun-Whe Kim","doi":"10.14701/kjhbps.2014.18.1.1","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Little is known about clinical features and survival outcome in locally advanced unresectable extrahepatic cholangiocarcinoma (EHC). The aim was to investigate the clinical features and the survival outcome in these patients, and to evaluate the role of palliative resections in locally advanced unresectable EHC.</p><p><strong>Methods: </strong>Between 1995 and 2007, 280 patients with locally advanced unresectable EHC were identified. Clinical, pathologic, and survival data were investigated. A comparative analysis was done between those who received palliative resection (PR) and those who were not operated on (NR).</p><p><strong>Results: </strong>The overall median survival of the study population was 10±1 months, and the 3- and 5-year survival rates (YSR) were 8.5% and 2.5%, respectively. The median survival, 3- and 5-YSR of PR were 23 months, 32.1% and 13.1%, respectively. For NR, they were 9 months, 3.9% and 0%, which were significantly worse than PR (p<0.001). In univariate analysis, T classification, N classification, tumor location, palliative resection, adjuvant treatment, chemotherapy, and radiation therapy were factors that showed survival difference between PR and NR. Regional lymph node metastasis (RR, 2.084; 95% CI, 1.491-2.914; p<0.001), non-resections (RR, 2.270; 95% CI, 1.497-3.443; p<0.001), and no chemotherapy (RR, 1.604; 95% CI, 1.095-2.349; p=0.015) were identified as risk factors for poor outcome on multivariate analysis.</p><p><strong>Conclusions: </strong>Without evidence of systemic disease, palliative resection may provide some survival benefit in selected locally advanced unresectable EHCs and adjuvant treatment may further improve survival outcome.</p>","PeriodicalId":91136,"journal":{"name":"Korean journal of hepato-biliary-pancreatic surgery","volume":"18 1","pages":"1-8"},"PeriodicalIF":0.0000,"publicationDate":"2014-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/70/kjhbps-18-1.PMC4492336.pdf","citationCount":"2","resultStr":"{\"title\":\"Clinical features and survival outcome of locally advanced extrahepatic cholangiocarcinoma.\",\"authors\":\"Sang-Jae Lee, Wooil Kwon, Mee Joo Kang, Jin-Young Jang, Ye Rim Chang, Woohyun Jung, Sun-Whe Kim\",\"doi\":\"10.14701/kjhbps.2014.18.1.1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Backgrounds/aims: </strong>Little is known about clinical features and survival outcome in locally advanced unresectable extrahepatic cholangiocarcinoma (EHC). The aim was to investigate the clinical features and the survival outcome in these patients, and to evaluate the role of palliative resections in locally advanced unresectable EHC.</p><p><strong>Methods: </strong>Between 1995 and 2007, 280 patients with locally advanced unresectable EHC were identified. Clinical, pathologic, and survival data were investigated. A comparative analysis was done between those who received palliative resection (PR) and those who were not operated on (NR).</p><p><strong>Results: </strong>The overall median survival of the study population was 10±1 months, and the 3- and 5-year survival rates (YSR) were 8.5% and 2.5%, respectively. The median survival, 3- and 5-YSR of PR were 23 months, 32.1% and 13.1%, respectively. For NR, they were 9 months, 3.9% and 0%, which were significantly worse than PR (p<0.001). In univariate analysis, T classification, N classification, tumor location, palliative resection, adjuvant treatment, chemotherapy, and radiation therapy were factors that showed survival difference between PR and NR. Regional lymph node metastasis (RR, 2.084; 95% CI, 1.491-2.914; p<0.001), non-resections (RR, 2.270; 95% CI, 1.497-3.443; p<0.001), and no chemotherapy (RR, 1.604; 95% CI, 1.095-2.349; p=0.015) were identified as risk factors for poor outcome on multivariate analysis.</p><p><strong>Conclusions: </strong>Without evidence of systemic disease, palliative resection may provide some survival benefit in selected locally advanced unresectable EHCs and adjuvant treatment may further improve survival outcome.</p>\",\"PeriodicalId\":91136,\"journal\":{\"name\":\"Korean journal of hepato-biliary-pancreatic surgery\",\"volume\":\"18 1\",\"pages\":\"1-8\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2014-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/70/kjhbps-18-1.PMC4492336.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean journal of hepato-biliary-pancreatic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14701/kjhbps.2014.18.1.1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/2/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean journal of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/kjhbps.2014.18.1.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/2/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Clinical features and survival outcome of locally advanced extrahepatic cholangiocarcinoma.
Backgrounds/aims: Little is known about clinical features and survival outcome in locally advanced unresectable extrahepatic cholangiocarcinoma (EHC). The aim was to investigate the clinical features and the survival outcome in these patients, and to evaluate the role of palliative resections in locally advanced unresectable EHC.
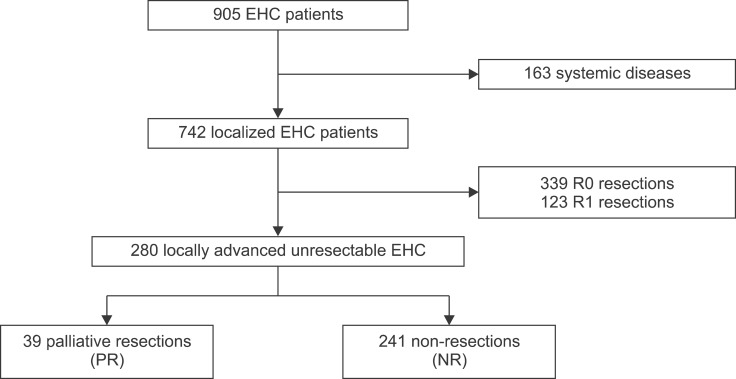
Methods: Between 1995 and 2007, 280 patients with locally advanced unresectable EHC were identified. Clinical, pathologic, and survival data were investigated. A comparative analysis was done between those who received palliative resection (PR) and those who were not operated on (NR).
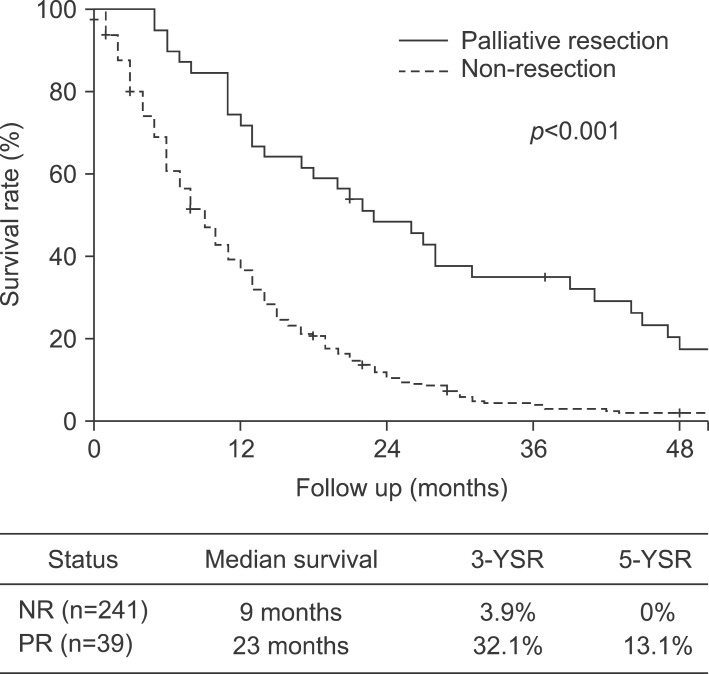
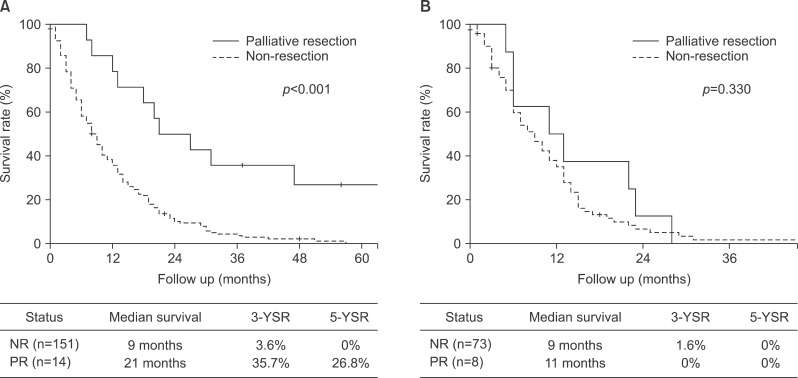
Results: The overall median survival of the study population was 10±1 months, and the 3- and 5-year survival rates (YSR) were 8.5% and 2.5%, respectively. The median survival, 3- and 5-YSR of PR were 23 months, 32.1% and 13.1%, respectively. For NR, they were 9 months, 3.9% and 0%, which were significantly worse than PR (p<0.001). In univariate analysis, T classification, N classification, tumor location, palliative resection, adjuvant treatment, chemotherapy, and radiation therapy were factors that showed survival difference between PR and NR. Regional lymph node metastasis (RR, 2.084; 95% CI, 1.491-2.914; p<0.001), non-resections (RR, 2.270; 95% CI, 1.497-3.443; p<0.001), and no chemotherapy (RR, 1.604; 95% CI, 1.095-2.349; p=0.015) were identified as risk factors for poor outcome on multivariate analysis.
Conclusions: Without evidence of systemic disease, palliative resection may provide some survival benefit in selected locally advanced unresectable EHCs and adjuvant treatment may further improve survival outcome.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
