Sung Hyun Kim, Hae Min Lee, Seung Ho Lee, Jong Yoon Won, Kyung Sik Kim
{"title":"病因不常见的门静脉高压症的处理。","authors":"Sung Hyun Kim, Hae Min Lee, Seung Ho Lee, Jong Yoon Won, Kyung Sik Kim","doi":"10.14701/kjhbps.2016.20.2.81","DOIUrl":null,"url":null,"abstract":"<p><p>Portal hypertension can arise from any condition interfering with normal blood flow at any level within the portal system. Herein, we presented two uncommon cases of the portal hypertension and its treatment with brief literature review. A 71-year-old man who underwent right hemihepatectomy revealed a tumor recurrence adjacent to the inferior vena cava (IVC). After radiofrequency ablation (RFA) with lymph node dissection, he was referred for abdominal distension. The abdomen computed tomography scan showed severe ascites with a narrowing middle hepatic vein (MHV) and IVC around the RFA site. After insertion of two stents at the IVC and MHV, the ascites disappeared. Another 73-year-old man underwent right trisectionectomy of liver and segmental resection of the portal vein (PV). After operation, he underwent conservative management due to continuous abdominal ascites. The abdomen computed tomography scan showed severe ascites with obliteration of the left PV. After insertion of stent, the ascites disappeared. A decrease of the pressure gradient between the PV and IVC is one of the important treatment strategies for portal hypertension. Vascular stent is useful in the reduction of pressure gradient and thus, can be a treatment option for portal hypertension. </p>","PeriodicalId":91136,"journal":{"name":"Korean journal of hepato-biliary-pancreatic surgery","volume":"20 2","pages":"81-4"},"PeriodicalIF":0.0000,"publicationDate":"2016-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.14701/kjhbps.2016.20.2.81","citationCount":"0","resultStr":"{\"title\":\"Management of portal hypertension derived from uncommon causes.\",\"authors\":\"Sung Hyun Kim, Hae Min Lee, Seung Ho Lee, Jong Yoon Won, Kyung Sik Kim\",\"doi\":\"10.14701/kjhbps.2016.20.2.81\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Portal hypertension can arise from any condition interfering with normal blood flow at any level within the portal system. Herein, we presented two uncommon cases of the portal hypertension and its treatment with brief literature review. A 71-year-old man who underwent right hemihepatectomy revealed a tumor recurrence adjacent to the inferior vena cava (IVC). After radiofrequency ablation (RFA) with lymph node dissection, he was referred for abdominal distension. The abdomen computed tomography scan showed severe ascites with a narrowing middle hepatic vein (MHV) and IVC around the RFA site. After insertion of two stents at the IVC and MHV, the ascites disappeared. Another 73-year-old man underwent right trisectionectomy of liver and segmental resection of the portal vein (PV). After operation, he underwent conservative management due to continuous abdominal ascites. The abdomen computed tomography scan showed severe ascites with obliteration of the left PV. After insertion of stent, the ascites disappeared. A decrease of the pressure gradient between the PV and IVC is one of the important treatment strategies for portal hypertension. Vascular stent is useful in the reduction of pressure gradient and thus, can be a treatment option for portal hypertension. </p>\",\"PeriodicalId\":91136,\"journal\":{\"name\":\"Korean journal of hepato-biliary-pancreatic surgery\",\"volume\":\"20 2\",\"pages\":\"81-4\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.14701/kjhbps.2016.20.2.81\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean journal of hepato-biliary-pancreatic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14701/kjhbps.2016.20.2.81\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/5/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean journal of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/kjhbps.2016.20.2.81","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/5/11 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Management of portal hypertension derived from uncommon causes.
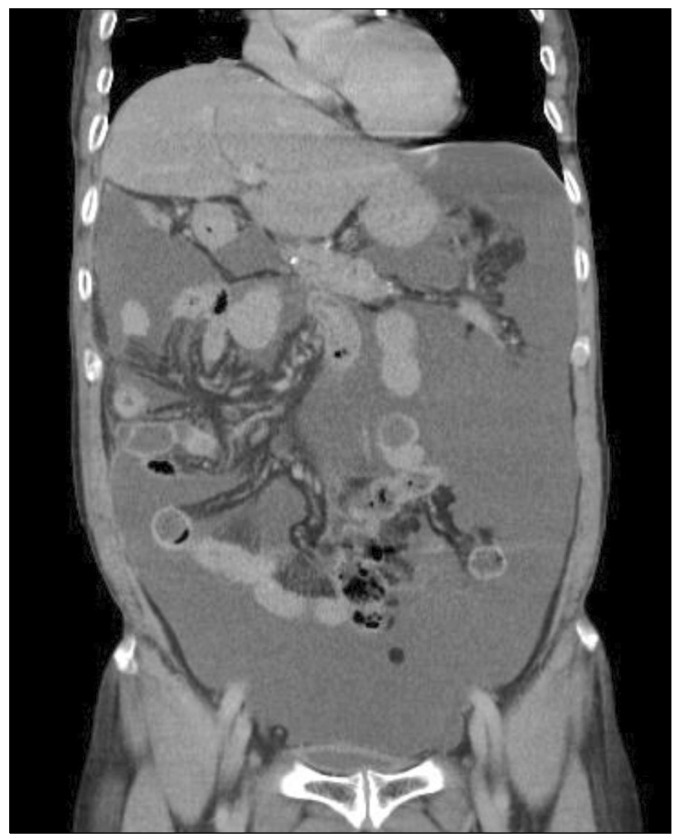
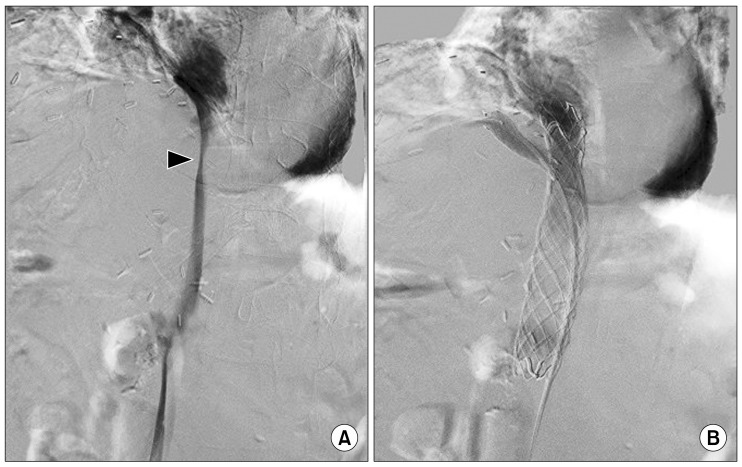
Portal hypertension can arise from any condition interfering with normal blood flow at any level within the portal system. Herein, we presented two uncommon cases of the portal hypertension and its treatment with brief literature review. A 71-year-old man who underwent right hemihepatectomy revealed a tumor recurrence adjacent to the inferior vena cava (IVC). After radiofrequency ablation (RFA) with lymph node dissection, he was referred for abdominal distension. The abdomen computed tomography scan showed severe ascites with a narrowing middle hepatic vein (MHV) and IVC around the RFA site. After insertion of two stents at the IVC and MHV, the ascites disappeared. Another 73-year-old man underwent right trisectionectomy of liver and segmental resection of the portal vein (PV). After operation, he underwent conservative management due to continuous abdominal ascites. The abdomen computed tomography scan showed severe ascites with obliteration of the left PV. After insertion of stent, the ascites disappeared. A decrease of the pressure gradient between the PV and IVC is one of the important treatment strategies for portal hypertension. Vascular stent is useful in the reduction of pressure gradient and thus, can be a treatment option for portal hypertension.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
