{"title":"成人急性肾损伤患者连续和间歇肾替代治疗的效果。","authors":"Tonio Schoenfelder, Xiaoyu Chen, Hans-Holger Bleß","doi":"10.3205/hta000127","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Dialysis-dependent acute kidney injury (AKI) can be treated using continuous (CRRT) or intermittent renal replacement therapies (IRRT). Although some studies suggest that CRRT may have advantages over IRRT, study findings are inconsistent. This study assessed differences between CRRT and IRRT regarding important clinical outcomes (such as mortality and renal recovery) and cost-effectiveness. Additionally, ethical aspects that are linked to renal replacement therapies in the intensive care setting are considered. <b>Methods:</b> Systematic searches in MEDLINE, EMBASE, and Cochrane Library including RCTs, observational studies, and cost-effectiveness studies were performed. Results were pooled using a random effects-model. <b>Results:</b> Forty-nine studies were included. Findings show a higher rate of renal recovery among survivors who initially received CRRT as compared with IRRT. This advantage applies to the analysis of all studies with different observation periods (Relative Risk (RR) 1.10; 95% Confidence Interval (CI) [1.05, 1.16]) and to a selection of studies with observation periods of 90 days (RR 1.07; 95% CI [1.04, 1.09]). Regarding observation periods beyond there are no differences when only two identified studies were analyzed. Patients initially receiving CRRT have higher mortality as compared to IRRT (RR 1.17; 95% CI [1.06, 1.28]). This difference is attributable to observational studies and may have been caused by allocation bias since seriously ill patients more often initially receive CRRT instead of IRRT. CRRT do not significantly differ from IRRT with respect to change of mean arterial pressure, hypotensive episodes, hemodynamic instability, and length of stay. Data on cost-effectiveness is inconsistent. Recent analyzes indicate that initial CRRT is cost-effective compared to initial IRRT due to a reduction of the rate of long-term dialysis dependence. As regards a short time horizon, this cost benefit has not been shown. <b>Conclusion:</b> Findings of the conducted assessment show that initial CRRT is associated with higher rates of renal recovery. Potential long-term effects on clinical outcomes for more than three months could not be analyzed and should be investigated in further studies. Economical analyzes indicate that initial CRRT is cost-effective when costs of long-term dialysis dependence are considered. However, transferability of the economic analyzes to the German health care system is limited and the conduction of economical analyzes using national cost data should be considered.</p>","PeriodicalId":89142,"journal":{"name":"GMS health technology assessment","volume":"13 ","pages":"Doc01"},"PeriodicalIF":0.0000,"publicationDate":"2017-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.3205/hta000127","citationCount":"15","resultStr":"{\"title\":\"Effects of continuous and intermittent renal replacement therapies among adult patients with acute kidney injury.\",\"authors\":\"Tonio Schoenfelder, Xiaoyu Chen, Hans-Holger Bleß\",\"doi\":\"10.3205/hta000127\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Dialysis-dependent acute kidney injury (AKI) can be treated using continuous (CRRT) or intermittent renal replacement therapies (IRRT). Although some studies suggest that CRRT may have advantages over IRRT, study findings are inconsistent. This study assessed differences between CRRT and IRRT regarding important clinical outcomes (such as mortality and renal recovery) and cost-effectiveness. Additionally, ethical aspects that are linked to renal replacement therapies in the intensive care setting are considered. <b>Methods:</b> Systematic searches in MEDLINE, EMBASE, and Cochrane Library including RCTs, observational studies, and cost-effectiveness studies were performed. Results were pooled using a random effects-model. <b>Results:</b> Forty-nine studies were included. Findings show a higher rate of renal recovery among survivors who initially received CRRT as compared with IRRT. This advantage applies to the analysis of all studies with different observation periods (Relative Risk (RR) 1.10; 95% Confidence Interval (CI) [1.05, 1.16]) and to a selection of studies with observation periods of 90 days (RR 1.07; 95% CI [1.04, 1.09]). Regarding observation periods beyond there are no differences when only two identified studies were analyzed. Patients initially receiving CRRT have higher mortality as compared to IRRT (RR 1.17; 95% CI [1.06, 1.28]). This difference is attributable to observational studies and may have been caused by allocation bias since seriously ill patients more often initially receive CRRT instead of IRRT. CRRT do not significantly differ from IRRT with respect to change of mean arterial pressure, hypotensive episodes, hemodynamic instability, and length of stay. Data on cost-effectiveness is inconsistent. Recent analyzes indicate that initial CRRT is cost-effective compared to initial IRRT due to a reduction of the rate of long-term dialysis dependence. As regards a short time horizon, this cost benefit has not been shown. <b>Conclusion:</b> Findings of the conducted assessment show that initial CRRT is associated with higher rates of renal recovery. Potential long-term effects on clinical outcomes for more than three months could not be analyzed and should be investigated in further studies. Economical analyzes indicate that initial CRRT is cost-effective when costs of long-term dialysis dependence are considered. However, transferability of the economic analyzes to the German health care system is limited and the conduction of economical analyzes using national cost data should be considered.</p>\",\"PeriodicalId\":89142,\"journal\":{\"name\":\"GMS health technology assessment\",\"volume\":\"13 \",\"pages\":\"Doc01\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.3205/hta000127\",\"citationCount\":\"15\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GMS health technology assessment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3205/hta000127\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS health technology assessment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/hta000127","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Effects of continuous and intermittent renal replacement therapies among adult patients with acute kidney injury.
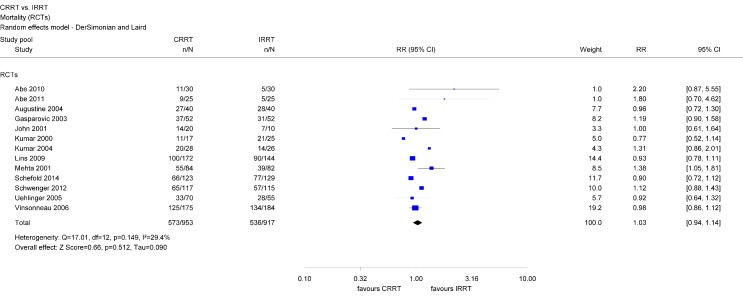
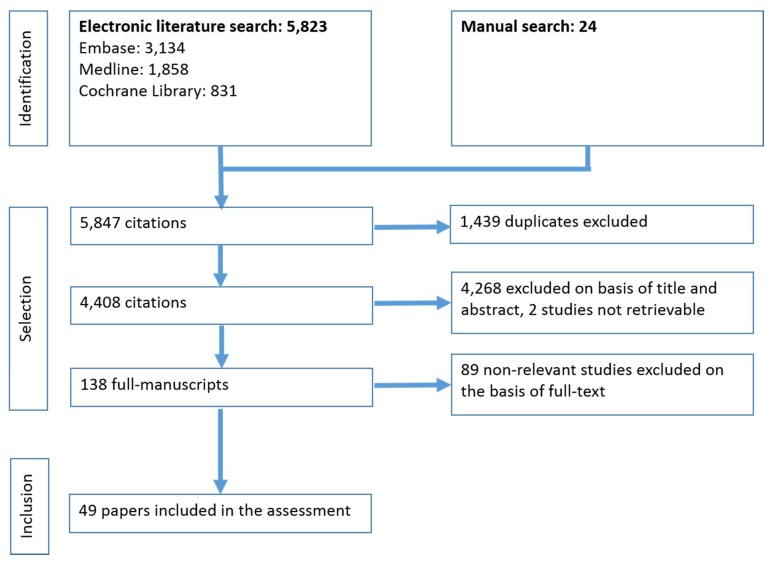
Background: Dialysis-dependent acute kidney injury (AKI) can be treated using continuous (CRRT) or intermittent renal replacement therapies (IRRT). Although some studies suggest that CRRT may have advantages over IRRT, study findings are inconsistent. This study assessed differences between CRRT and IRRT regarding important clinical outcomes (such as mortality and renal recovery) and cost-effectiveness. Additionally, ethical aspects that are linked to renal replacement therapies in the intensive care setting are considered. Methods: Systematic searches in MEDLINE, EMBASE, and Cochrane Library including RCTs, observational studies, and cost-effectiveness studies were performed. Results were pooled using a random effects-model. Results: Forty-nine studies were included. Findings show a higher rate of renal recovery among survivors who initially received CRRT as compared with IRRT. This advantage applies to the analysis of all studies with different observation periods (Relative Risk (RR) 1.10; 95% Confidence Interval (CI) [1.05, 1.16]) and to a selection of studies with observation periods of 90 days (RR 1.07; 95% CI [1.04, 1.09]). Regarding observation periods beyond there are no differences when only two identified studies were analyzed. Patients initially receiving CRRT have higher mortality as compared to IRRT (RR 1.17; 95% CI [1.06, 1.28]). This difference is attributable to observational studies and may have been caused by allocation bias since seriously ill patients more often initially receive CRRT instead of IRRT. CRRT do not significantly differ from IRRT with respect to change of mean arterial pressure, hypotensive episodes, hemodynamic instability, and length of stay. Data on cost-effectiveness is inconsistent. Recent analyzes indicate that initial CRRT is cost-effective compared to initial IRRT due to a reduction of the rate of long-term dialysis dependence. As regards a short time horizon, this cost benefit has not been shown. Conclusion: Findings of the conducted assessment show that initial CRRT is associated with higher rates of renal recovery. Potential long-term effects on clinical outcomes for more than three months could not be analyzed and should be investigated in further studies. Economical analyzes indicate that initial CRRT is cost-effective when costs of long-term dialysis dependence are considered. However, transferability of the economic analyzes to the German health care system is limited and the conduction of economical analyzes using national cost data should be considered.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
