Hanoon P Pokharel, Neville F Hacker, Lesley Andrews
{"title":"改善妇科肿瘤患者的遗传咨询服务。","authors":"Hanoon P Pokharel, Neville F Hacker, Lesley Andrews","doi":"10.1186/s40661-018-0059-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Gynaecological cancers may be the sentinel malignancy in women who carry a mutation in BRCA1 or 2, a mis-match repair gene causing Lynch Syndrome or other genes. Despite published guidelines for referral to a genetics service, a substantial number of women do not attend for the recommended genetic assessment. The study aims to determine the outcomes of systematic follow-up of patients diagnosed with ovarian or endometrial cancer from Gynaecologic-oncology multidisciplinary meetings who were deemed appropriate for genetics assessment.</p><p><strong>Methods: </strong>Women newly diagnosed with gynaecological cancer at the Royal Hospital for Women between 2010 and 2014 (cohort1) and 2015-2016 (cohort 2) who were identified as suitable for genetics assessment were checked against the New South Wales/Australian Capital Territory genetic database. The doctors of non-attenders were contacted regarding suitability for re-referral, and patients who were still suitable for genetics assessment were contacted by mail. Attendance was again checked against the genetics database.</p><p><strong>Results: </strong>Among 462 patients in cohort 1, flagged for genetic assessment, 167 had not consulted a genetic service at initial audit conducted in 2014. 86 (18.6%) women whose referral was pending clarification of family history and/or immunohistochemistry did not require further genetic assessment. Letters were sent to 40 women. 7 women (1.5%) attended hereditary cancer clinic in the following 6 months.The audit conducted in 2016 identified 148 patients (cohort 2) appropriate for genetic assessment at diagnosis. 66 (44.6%) had been seen by a genetics service, 51 (34.5%) whose referral was pending additional information did not require further genetic assessment. Letters were sent to 15 women, of whom 9 (6.1%) attended genetics within 6 months.</p><p><strong>Conclusions: </strong>To improve the effectiveness of guidelines for the genetic referral of women newly diagnosed with ovarian cancer, clinicians need to obtain a thorough family history at diagnosis; arrange for reflex MMR IHC according to guidelines; offer BRCA or panel testing to all women with non-mucinous ovarian cancer prior to discharge and systematically follow up all women referred to genetics at the post-op visit.</p>","PeriodicalId":91487,"journal":{"name":"Gynecologic oncology research and practice","volume":"5 ","pages":"2"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40661-018-0059-z","citationCount":"2","resultStr":"{\"title\":\"Improving attendance to genetic counselling services for gynaecological oncology patients.\",\"authors\":\"Hanoon P Pokharel, Neville F Hacker, Lesley Andrews\",\"doi\":\"10.1186/s40661-018-0059-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Gynaecological cancers may be the sentinel malignancy in women who carry a mutation in BRCA1 or 2, a mis-match repair gene causing Lynch Syndrome or other genes. Despite published guidelines for referral to a genetics service, a substantial number of women do not attend for the recommended genetic assessment. The study aims to determine the outcomes of systematic follow-up of patients diagnosed with ovarian or endometrial cancer from Gynaecologic-oncology multidisciplinary meetings who were deemed appropriate for genetics assessment.</p><p><strong>Methods: </strong>Women newly diagnosed with gynaecological cancer at the Royal Hospital for Women between 2010 and 2014 (cohort1) and 2015-2016 (cohort 2) who were identified as suitable for genetics assessment were checked against the New South Wales/Australian Capital Territory genetic database. The doctors of non-attenders were contacted regarding suitability for re-referral, and patients who were still suitable for genetics assessment were contacted by mail. Attendance was again checked against the genetics database.</p><p><strong>Results: </strong>Among 462 patients in cohort 1, flagged for genetic assessment, 167 had not consulted a genetic service at initial audit conducted in 2014. 86 (18.6%) women whose referral was pending clarification of family history and/or immunohistochemistry did not require further genetic assessment. Letters were sent to 40 women. 7 women (1.5%) attended hereditary cancer clinic in the following 6 months.The audit conducted in 2016 identified 148 patients (cohort 2) appropriate for genetic assessment at diagnosis. 66 (44.6%) had been seen by a genetics service, 51 (34.5%) whose referral was pending additional information did not require further genetic assessment. Letters were sent to 15 women, of whom 9 (6.1%) attended genetics within 6 months.</p><p><strong>Conclusions: </strong>To improve the effectiveness of guidelines for the genetic referral of women newly diagnosed with ovarian cancer, clinicians need to obtain a thorough family history at diagnosis; arrange for reflex MMR IHC according to guidelines; offer BRCA or panel testing to all women with non-mucinous ovarian cancer prior to discharge and systematically follow up all women referred to genetics at the post-op visit.</p>\",\"PeriodicalId\":91487,\"journal\":{\"name\":\"Gynecologic oncology research and practice\",\"volume\":\"5 \",\"pages\":\"2\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-01-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s40661-018-0059-z\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gynecologic oncology research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40661-018-0059-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecologic oncology research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40661-018-0059-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Improving attendance to genetic counselling services for gynaecological oncology patients.
Background: Gynaecological cancers may be the sentinel malignancy in women who carry a mutation in BRCA1 or 2, a mis-match repair gene causing Lynch Syndrome or other genes. Despite published guidelines for referral to a genetics service, a substantial number of women do not attend for the recommended genetic assessment. The study aims to determine the outcomes of systematic follow-up of patients diagnosed with ovarian or endometrial cancer from Gynaecologic-oncology multidisciplinary meetings who were deemed appropriate for genetics assessment.
Methods: Women newly diagnosed with gynaecological cancer at the Royal Hospital for Women between 2010 and 2014 (cohort1) and 2015-2016 (cohort 2) who were identified as suitable for genetics assessment were checked against the New South Wales/Australian Capital Territory genetic database. The doctors of non-attenders were contacted regarding suitability for re-referral, and patients who were still suitable for genetics assessment were contacted by mail. Attendance was again checked against the genetics database.
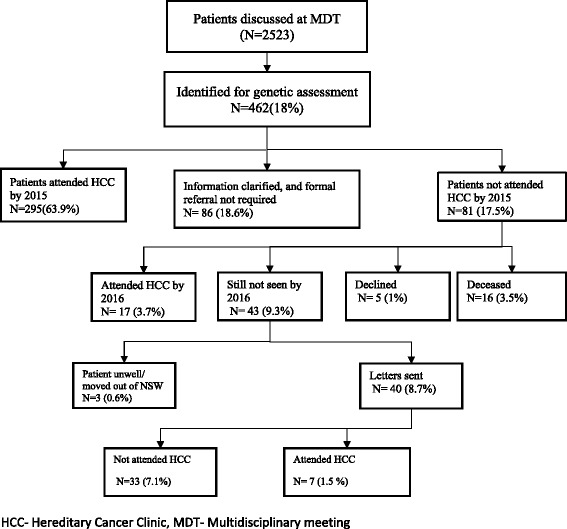
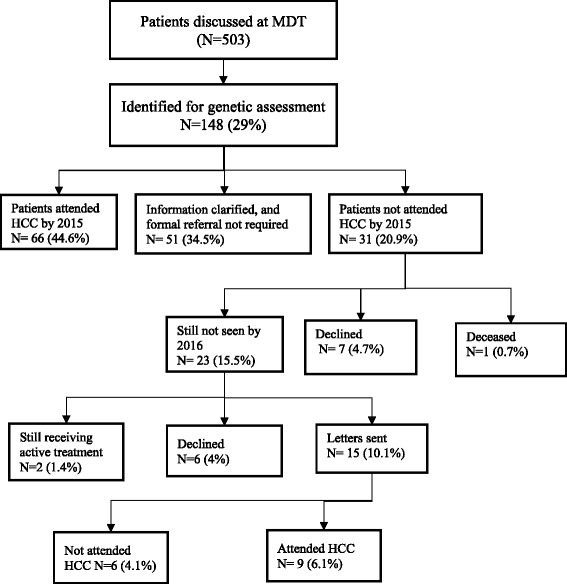
Results: Among 462 patients in cohort 1, flagged for genetic assessment, 167 had not consulted a genetic service at initial audit conducted in 2014. 86 (18.6%) women whose referral was pending clarification of family history and/or immunohistochemistry did not require further genetic assessment. Letters were sent to 40 women. 7 women (1.5%) attended hereditary cancer clinic in the following 6 months.The audit conducted in 2016 identified 148 patients (cohort 2) appropriate for genetic assessment at diagnosis. 66 (44.6%) had been seen by a genetics service, 51 (34.5%) whose referral was pending additional information did not require further genetic assessment. Letters were sent to 15 women, of whom 9 (6.1%) attended genetics within 6 months.
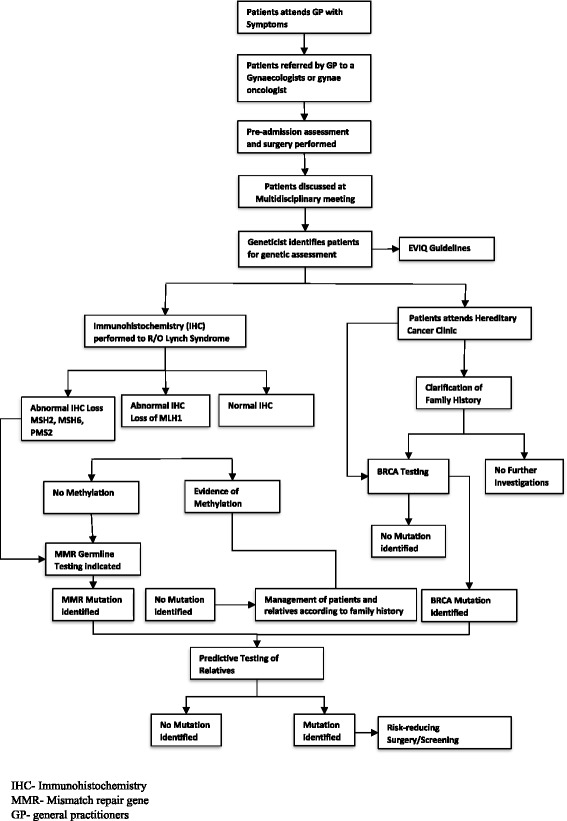
Conclusions: To improve the effectiveness of guidelines for the genetic referral of women newly diagnosed with ovarian cancer, clinicians need to obtain a thorough family history at diagnosis; arrange for reflex MMR IHC according to guidelines; offer BRCA or panel testing to all women with non-mucinous ovarian cancer prior to discharge and systematically follow up all women referred to genetics at the post-op visit.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
