{"title":"PCSK9抑制剂和他汀类药物联合治疗冠状动脉钙化的年发生率低于他汀类药物单药治疗。","authors":"Yuichi Ikegami, Ikuo Inoue, Kaiji Inoue, Yuichi Shinoda, Shinichiro Iida, Seiichi Goto, Takanari Nakano, Akira Shimada, Mistuhiko Noda","doi":"10.1038/s41514-018-0026-2","DOIUrl":null,"url":null,"abstract":"<p><p>Statins and/or PCSK9 inhibitors cause the regression of coronary atheroma and reduce clinical events. However, it currently remains unclear whether these drugs modulate coronary atheroma calcification in vivo. Coronary artery calcium (CAC) scores (Agatston Units, AUs) were estimated in 120 patients receiving coronary computed tomographic angiography (CCTA) (63% males; median age 56 years). The CAC scores were compared among the three groups: (1) neither statin nor PCSK9 inhibitor therapy, (2) statin monotherapy, and (3) statin and PCSK9 inhibitor combination therapy in an unpaired cross-sectional study. Additionally, CCTA was performed twice at an interval in 15 patients undergoing statin monotherapy to compare the previous (baseline) and subsequent (follow-up) CAC scores in a paired longitudinal study. In addition, a PCSK9 inhibitor was administered to 16 patients undergoing statin therapy. Before and after that, CCTA was performed twice to compare the previous and subsequent CAC scores in a paired longitudinal study. The unpaired cross-sectional study and paired longitudinal study consist of completely different patients. Among 120 patients, 40 (33%) had a CAC score >100 AUs. The median CAC score increased in the following order: statin group, statin and PCSK9 group, and no-statin-no-PCSK9 group. Annual CAC score progression was 29.7% by statin monotherapy and 14.3% following the addition of the PCSK9 inhibitor to statin therapy. The annual rate of CAC with the combination therapy with a PCSK9 inhibitor and a statin is lower than that with statin monotherapy. CAC may be prevented with PCSK9 Inhibitor.</p>","PeriodicalId":5,"journal":{"name":"ACS Applied Materials & Interfaces","volume":" ","pages":"7"},"PeriodicalIF":8.2000,"publicationDate":"2018-06-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6015059/pdf/","citationCount":"0","resultStr":"{\"title\":\"The annual rate of coronary artery calcification with combination therapy with a PCSK9 inhibitor and a statin is lower than that with statin monotherapy.\",\"authors\":\"Yuichi Ikegami, Ikuo Inoue, Kaiji Inoue, Yuichi Shinoda, Shinichiro Iida, Seiichi Goto, Takanari Nakano, Akira Shimada, Mistuhiko Noda\",\"doi\":\"10.1038/s41514-018-0026-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Statins and/or PCSK9 inhibitors cause the regression of coronary atheroma and reduce clinical events. However, it currently remains unclear whether these drugs modulate coronary atheroma calcification in vivo. Coronary artery calcium (CAC) scores (Agatston Units, AUs) were estimated in 120 patients receiving coronary computed tomographic angiography (CCTA) (63% males; median age 56 years). The CAC scores were compared among the three groups: (1) neither statin nor PCSK9 inhibitor therapy, (2) statin monotherapy, and (3) statin and PCSK9 inhibitor combination therapy in an unpaired cross-sectional study. Additionally, CCTA was performed twice at an interval in 15 patients undergoing statin monotherapy to compare the previous (baseline) and subsequent (follow-up) CAC scores in a paired longitudinal study. In addition, a PCSK9 inhibitor was administered to 16 patients undergoing statin therapy. Before and after that, CCTA was performed twice to compare the previous and subsequent CAC scores in a paired longitudinal study. The unpaired cross-sectional study and paired longitudinal study consist of completely different patients. Among 120 patients, 40 (33%) had a CAC score >100 AUs. The median CAC score increased in the following order: statin group, statin and PCSK9 group, and no-statin-no-PCSK9 group. Annual CAC score progression was 29.7% by statin monotherapy and 14.3% following the addition of the PCSK9 inhibitor to statin therapy. The annual rate of CAC with the combination therapy with a PCSK9 inhibitor and a statin is lower than that with statin monotherapy. CAC may be prevented with PCSK9 Inhibitor.</p>\",\"PeriodicalId\":5,\"journal\":{\"name\":\"ACS Applied Materials & Interfaces\",\"volume\":\" \",\"pages\":\"7\"},\"PeriodicalIF\":8.2000,\"publicationDate\":\"2018-06-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6015059/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Materials & Interfaces\",\"FirstCategoryId\":\"88\",\"ListUrlMain\":\"https://doi.org/10.1038/s41514-018-0026-2\",\"RegionNum\":2,\"RegionCategory\":\"材料科学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MATERIALS SCIENCE, MULTIDISCIPLINARY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Materials & Interfaces","FirstCategoryId":"88","ListUrlMain":"https://doi.org/10.1038/s41514-018-0026-2","RegionNum":2,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MATERIALS SCIENCE, MULTIDISCIPLINARY","Score":null,"Total":0}
The annual rate of coronary artery calcification with combination therapy with a PCSK9 inhibitor and a statin is lower than that with statin monotherapy.
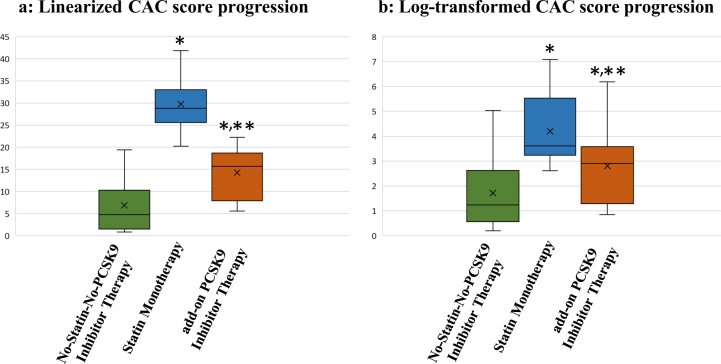
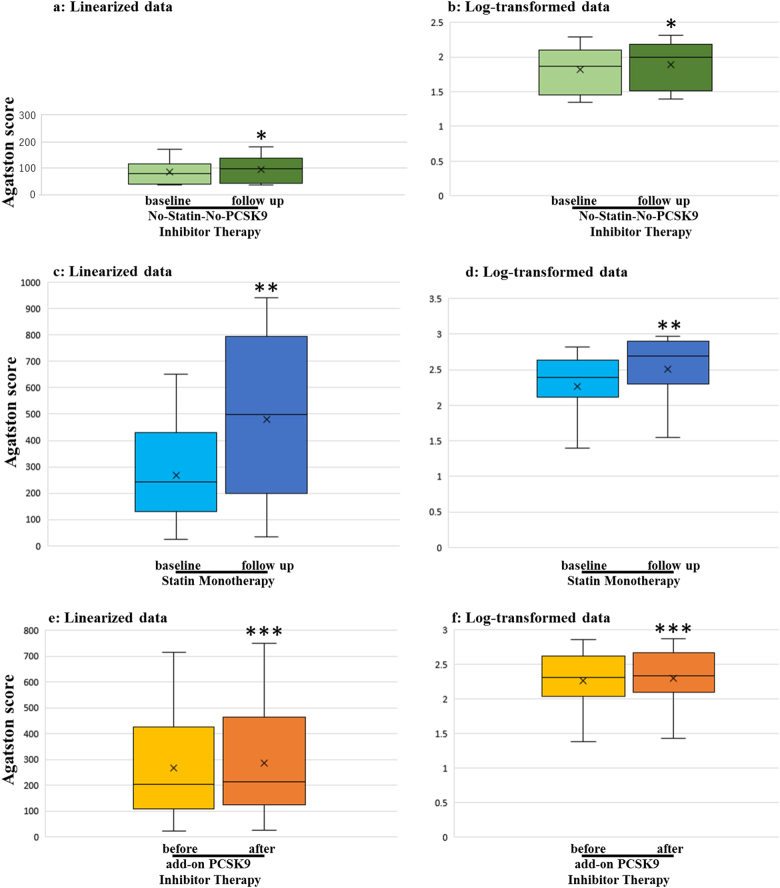
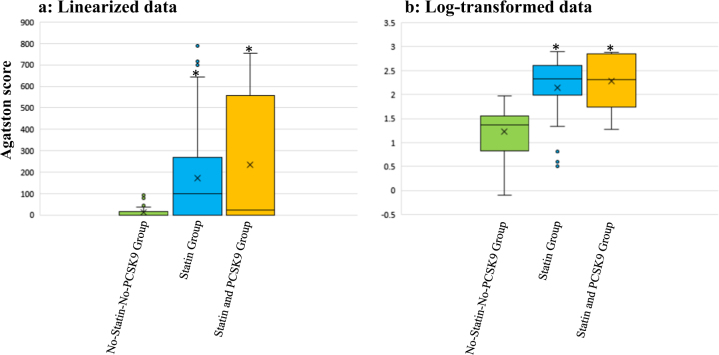
Statins and/or PCSK9 inhibitors cause the regression of coronary atheroma and reduce clinical events. However, it currently remains unclear whether these drugs modulate coronary atheroma calcification in vivo. Coronary artery calcium (CAC) scores (Agatston Units, AUs) were estimated in 120 patients receiving coronary computed tomographic angiography (CCTA) (63% males; median age 56 years). The CAC scores were compared among the three groups: (1) neither statin nor PCSK9 inhibitor therapy, (2) statin monotherapy, and (3) statin and PCSK9 inhibitor combination therapy in an unpaired cross-sectional study. Additionally, CCTA was performed twice at an interval in 15 patients undergoing statin monotherapy to compare the previous (baseline) and subsequent (follow-up) CAC scores in a paired longitudinal study. In addition, a PCSK9 inhibitor was administered to 16 patients undergoing statin therapy. Before and after that, CCTA was performed twice to compare the previous and subsequent CAC scores in a paired longitudinal study. The unpaired cross-sectional study and paired longitudinal study consist of completely different patients. Among 120 patients, 40 (33%) had a CAC score >100 AUs. The median CAC score increased in the following order: statin group, statin and PCSK9 group, and no-statin-no-PCSK9 group. Annual CAC score progression was 29.7% by statin monotherapy and 14.3% following the addition of the PCSK9 inhibitor to statin therapy. The annual rate of CAC with the combination therapy with a PCSK9 inhibitor and a statin is lower than that with statin monotherapy. CAC may be prevented with PCSK9 Inhibitor.
期刊介绍:
ACS Applied Materials & Interfaces is a leading interdisciplinary journal that brings together chemists, engineers, physicists, and biologists to explore the development and utilization of newly-discovered materials and interfacial processes for specific applications. Our journal has experienced remarkable growth since its establishment in 2009, both in terms of the number of articles published and the impact of the research showcased. We are proud to foster a truly global community, with the majority of published articles originating from outside the United States, reflecting the rapid growth of applied research worldwide.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
