{"title":"托伐普坦治疗心力衰竭患者肾功能对中期预后的影响。","authors":"Kensuke Fujioka, Sumio Mizuno, Taro Ichise, Takao Matsui, Hiroaki Hirase, Masato Yamaguchi, Takahiko Aoyama, Masakazu Yamagishi, Noboru Fujino, Masa-Aki Kawashiri, Kenshi Hayashi","doi":"10.1177/1753944718819064","DOIUrl":null,"url":null,"abstract":"<p><strong>Background:: </strong>Although tolvaptan, an electrolyte-free water diuretic for congestive heart failure (HF), is reported to have no effect on long-term mortality or HF-related morbidity, there may exist some subgroups of patients who may receive beneficial effect of tolvaptan. The purpose of this study was to identify clinical factors associated with mid-term effect of tolvaptan on clinical outcomes of patients who discharged after acute HF.</p><p><strong>Methods:: </strong>We retrospectively analyzed 140 patients (88 male; mean age, 77.1 ± 11.0 years) with acute HF who received tolvaptan (initial dose 8.6 ± 3.6 mg/day) during their hospitalization. They were divided into two groups according to how the tolvaptan was used at discharge; 77 in the tolvaptan-continued group and 63 in the discontinued group.</p><p><strong>Results:: </strong>The Cox proportional hazards model revealed that eGFR was the only independent predictor for the occurrence of mid-term cardiac events (composite of re-hospitalization due to HF and all-cause death; aHR = 0.9870, p = 0.02597). The Kaplan-Meier survival curves of the two groups demonstrated no difference in cumulative event-free rates. In the subgroup with preserved renal function at admission (eGFR ⩾ 30 ml/min/1.73 m<sup>2</sup>), the continuous use of tolvaptan increased composite events (aHR = 2.130, p = 0.02549).</p><p><strong>Conclusions:: </strong>The continuous use of tolvaptan after discharge did not affect mid-term cardiac events of HF overall but may be associated with increased cardiac events in the subgroup with preserved renal function. These findings suggest that the tolvaptan administration might need to be limited to treatment of in-hospital acute HF.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":" ","pages":"1753944718819064"},"PeriodicalIF":2.2000,"publicationDate":"2019-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1753944718819064","citationCount":"1","resultStr":"{\"title\":\"Impact of renal function on mid-term outcomes in heart failure patients treated with tolvaptan.\",\"authors\":\"Kensuke Fujioka, Sumio Mizuno, Taro Ichise, Takao Matsui, Hiroaki Hirase, Masato Yamaguchi, Takahiko Aoyama, Masakazu Yamagishi, Noboru Fujino, Masa-Aki Kawashiri, Kenshi Hayashi\",\"doi\":\"10.1177/1753944718819064\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background:: </strong>Although tolvaptan, an electrolyte-free water diuretic for congestive heart failure (HF), is reported to have no effect on long-term mortality or HF-related morbidity, there may exist some subgroups of patients who may receive beneficial effect of tolvaptan. The purpose of this study was to identify clinical factors associated with mid-term effect of tolvaptan on clinical outcomes of patients who discharged after acute HF.</p><p><strong>Methods:: </strong>We retrospectively analyzed 140 patients (88 male; mean age, 77.1 ± 11.0 years) with acute HF who received tolvaptan (initial dose 8.6 ± 3.6 mg/day) during their hospitalization. They were divided into two groups according to how the tolvaptan was used at discharge; 77 in the tolvaptan-continued group and 63 in the discontinued group.</p><p><strong>Results:: </strong>The Cox proportional hazards model revealed that eGFR was the only independent predictor for the occurrence of mid-term cardiac events (composite of re-hospitalization due to HF and all-cause death; aHR = 0.9870, p = 0.02597). The Kaplan-Meier survival curves of the two groups demonstrated no difference in cumulative event-free rates. In the subgroup with preserved renal function at admission (eGFR ⩾ 30 ml/min/1.73 m<sup>2</sup>), the continuous use of tolvaptan increased composite events (aHR = 2.130, p = 0.02549).</p><p><strong>Conclusions:: </strong>The continuous use of tolvaptan after discharge did not affect mid-term cardiac events of HF overall but may be associated with increased cardiac events in the subgroup with preserved renal function. These findings suggest that the tolvaptan administration might need to be limited to treatment of in-hospital acute HF.</p>\",\"PeriodicalId\":23035,\"journal\":{\"name\":\"Therapeutic Advances in Cardiovascular Disease\",\"volume\":\" \",\"pages\":\"1753944718819064\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2019-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1753944718819064\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1753944718819064\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1753944718819064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
摘要
背景:虽然托伐普坦是一种无电解质水利尿剂,用于治疗充血性心力衰竭(HF),据报道对长期死亡率或HF相关发病率没有影响,但可能存在一些亚组的患者可能受益于托伐普坦。本研究的目的是确定与托伐普坦对急性心衰出院患者临床结局中期影响相关的临床因素。方法回顾性分析140例患者的临床资料,其中男性88例;平均年龄77.1±11.0岁),住院期间接受托伐普坦(初始剂量8.6±3.6 mg/天)治疗的急性HF患者。根据他们出院时使用托伐普坦的方式分为两组;托伐普坦继续组77例,停药组63例。结果:Cox比例风险模型显示,eGFR是中期心脏事件发生的唯一独立预测因子(合并HF再住院和全因死亡;aHR = 0.9870, p = 0.02597)。Kaplan-Meier生存曲线显示两组的累积无事件发生率无差异。在入院时肾功能保留的亚组(eGFR大于或等于30 ml/min/1.73 m2)中,持续使用托伐普坦增加了复合事件(aHR = 2.130, p = 0.02549)。结论:出院后继续使用托伐普坦对HF中期心脏事件总体上没有影响,但可能与肾功能保留亚组心脏事件增加有关。这些发现表明,托伐普坦可能需要限制在治疗院内急性心衰。
Impact of renal function on mid-term outcomes in heart failure patients treated with tolvaptan.
Background:: Although tolvaptan, an electrolyte-free water diuretic for congestive heart failure (HF), is reported to have no effect on long-term mortality or HF-related morbidity, there may exist some subgroups of patients who may receive beneficial effect of tolvaptan. The purpose of this study was to identify clinical factors associated with mid-term effect of tolvaptan on clinical outcomes of patients who discharged after acute HF.
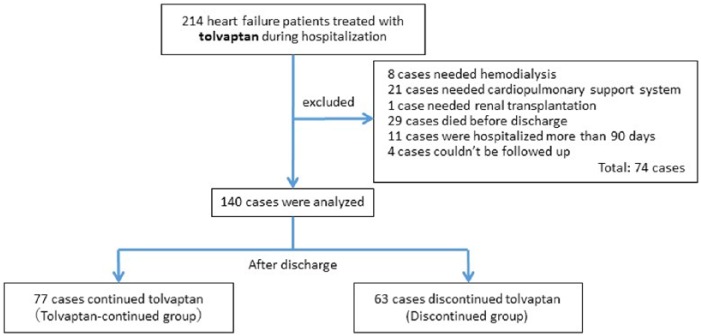
Methods:: We retrospectively analyzed 140 patients (88 male; mean age, 77.1 ± 11.0 years) with acute HF who received tolvaptan (initial dose 8.6 ± 3.6 mg/day) during their hospitalization. They were divided into two groups according to how the tolvaptan was used at discharge; 77 in the tolvaptan-continued group and 63 in the discontinued group.
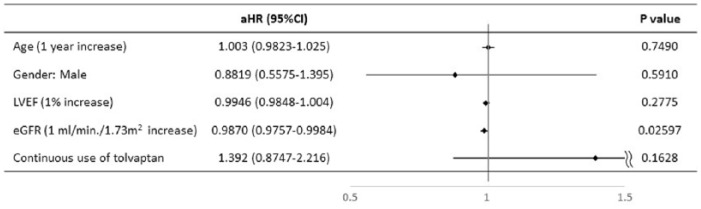
Results:: The Cox proportional hazards model revealed that eGFR was the only independent predictor for the occurrence of mid-term cardiac events (composite of re-hospitalization due to HF and all-cause death; aHR = 0.9870, p = 0.02597). The Kaplan-Meier survival curves of the two groups demonstrated no difference in cumulative event-free rates. In the subgroup with preserved renal function at admission (eGFR ⩾ 30 ml/min/1.73 m2), the continuous use of tolvaptan increased composite events (aHR = 2.130, p = 0.02549).
Conclusions:: The continuous use of tolvaptan after discharge did not affect mid-term cardiac events of HF overall but may be associated with increased cardiac events in the subgroup with preserved renal function. These findings suggest that the tolvaptan administration might need to be limited to treatment of in-hospital acute HF.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
