Alexander L Bisch, Courtney M Wheatley, Sarah E Baker, Elizabeth R Peitzman, Erik H Van Iterson, Theresa A Laguna, Wayne J Morgan, Eric M Snyder
{"title":"囊性纤维化跨膜传导调节基因型,而不是循环儿茶酚胺,影响囊性纤维化患者的心血管功能。","authors":"Alexander L Bisch, Courtney M Wheatley, Sarah E Baker, Elizabeth R Peitzman, Erik H Van Iterson, Theresa A Laguna, Wayne J Morgan, Eric M Snyder","doi":"10.1177/1179548419835788","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cystic fibrosis (CF) is a genetic disease affecting multiple organ systems of the body and is characterized by mutation in the gene coding for the cystic fibrosis transmembrane conductance regulator (CFTR). Previous work has shown that a single dose of aβ-agonist increases cardiac output (Q) and stroke volume (SV) and decreases systemic vascular resistance (SVR) in healthy subjects. This effect is attenuated in patients with CF; however, the mechanism is unknown. Potential explanations for this decreased cardiovascular response to a β-agonist in CF include inherent cardiovascular deficits secondary to the CFTR mutation, receptor desensitization from prolonged β-agonist use as part of clinical care, or inhibited drug delivery to the bloodstream due to mucus buildup in the lungs. This study sought to determine the effects of endogenous epinephrine (EPI) and norepinephrine (NE) on cardiovascular function in CF and to evaluate the relationship between cardiovascular function and CFTR F508del mutation.</p><p><strong>Methods: </strong>A total of 19 patients with CF and 31 healthy control subjects completed an assessment of Q (C<sub>2</sub>H<sub>2</sub> rebreathing), SV (calculated from Q and heart rate [HR]), Q and SV indexed to body surface area (BSA, QI, and SVI, respectively), SVR (through assessment of Q and mean arterial blood pressure [MAP]), and HR (from 12-lead electrocardiogram [ECG]) at rest along with plasma measures of EPI and NE. We compared subjects by variables of cardiovascular function relative to EPI and NE, and also based on genetic variants of the F508del mutation (homozygous deletion for F508del, heterozygous deletion for F508del, or no deletion of F508del).</p><p><strong>Results: </strong>Cystic fibrosis patients demonstrated significantly lower BSA (CF = 1.71 ± 0.05 m<sup>2</sup> vs healthy = 1.84 ± 0.04 m<sup>2</sup>, <i>P</i> = .03) and SVI (CF = 30.6 ± 2.5 mL/beat/m<sup>2</sup> vs healthy = 39.9 ± 2.5 mL/beat/m<sup>2</sup>, <i>P</i> = .02) when compared with healthy subjects. Cystic fibrosis patients also demonstrated lower Q (CF = 4.58 ± 0.36 L/min vs healthy = 5.71 ± 0.32 L/min, <i>P</i> = .03) and SV (CF = 54 ± 5.5 mL/beat vs healthy = 73.3 ± 4.5 mL/beat, <i>P</i> = .01), and a higher HR (CF = 93.2 ± 3.9 bpm vs healthy = 80.5 ± 2.7 bpm, <i>P</i> < .01) and SVR (CF = 2082 ± 156 dynes*s/cm<sup>-5</sup> vs healthy = 1616 ± 74 dynes*s/cm<sup>-5</sup>, <i>P</i> = .01) compared with healthy subjects. Furthermore, CF patients demonstrated a lower SV (<i>P</i> < .01) corrected for NE when compared with healthy subjects. No significant differences were seen in HR or Q relative to NE, or SVR relative to EPI. Differences were seen in SV (F<sub>(2,14)</sub> = 7.982, <i>P</i> < .01) and SV index (F<sub>(2,14)</sub> = 2.913, <i>P</i> = .08) when patients with CF were stratified according to F508del mutation (number of deletions).</p><p><strong>Conclusions: </strong>Individuals with CF have lower cardiac and peripheral hemodynamic function parameters at rest. Furthermore, these results suggest that impairment in cardiovascular function is likely the result of F508del CFTR genotype, rather than receptor desensitization or inhibited drug delivery.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"13 ","pages":"1179548419835788"},"PeriodicalIF":0.9000,"publicationDate":"2019-03-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179548419835788","citationCount":"5","resultStr":"{\"title\":\"Cystic Fibrosis Transmembrane Conductance Regulator Genotype, Not Circulating Catecholamines, Influences Cardiovascular Function in Patients with Cystic Fibrosis.\",\"authors\":\"Alexander L Bisch, Courtney M Wheatley, Sarah E Baker, Elizabeth R Peitzman, Erik H Van Iterson, Theresa A Laguna, Wayne J Morgan, Eric M Snyder\",\"doi\":\"10.1177/1179548419835788\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cystic fibrosis (CF) is a genetic disease affecting multiple organ systems of the body and is characterized by mutation in the gene coding for the cystic fibrosis transmembrane conductance regulator (CFTR). Previous work has shown that a single dose of aβ-agonist increases cardiac output (Q) and stroke volume (SV) and decreases systemic vascular resistance (SVR) in healthy subjects. This effect is attenuated in patients with CF; however, the mechanism is unknown. Potential explanations for this decreased cardiovascular response to a β-agonist in CF include inherent cardiovascular deficits secondary to the CFTR mutation, receptor desensitization from prolonged β-agonist use as part of clinical care, or inhibited drug delivery to the bloodstream due to mucus buildup in the lungs. This study sought to determine the effects of endogenous epinephrine (EPI) and norepinephrine (NE) on cardiovascular function in CF and to evaluate the relationship between cardiovascular function and CFTR F508del mutation.</p><p><strong>Methods: </strong>A total of 19 patients with CF and 31 healthy control subjects completed an assessment of Q (C<sub>2</sub>H<sub>2</sub> rebreathing), SV (calculated from Q and heart rate [HR]), Q and SV indexed to body surface area (BSA, QI, and SVI, respectively), SVR (through assessment of Q and mean arterial blood pressure [MAP]), and HR (from 12-lead electrocardiogram [ECG]) at rest along with plasma measures of EPI and NE. We compared subjects by variables of cardiovascular function relative to EPI and NE, and also based on genetic variants of the F508del mutation (homozygous deletion for F508del, heterozygous deletion for F508del, or no deletion of F508del).</p><p><strong>Results: </strong>Cystic fibrosis patients demonstrated significantly lower BSA (CF = 1.71 ± 0.05 m<sup>2</sup> vs healthy = 1.84 ± 0.04 m<sup>2</sup>, <i>P</i> = .03) and SVI (CF = 30.6 ± 2.5 mL/beat/m<sup>2</sup> vs healthy = 39.9 ± 2.5 mL/beat/m<sup>2</sup>, <i>P</i> = .02) when compared with healthy subjects. Cystic fibrosis patients also demonstrated lower Q (CF = 4.58 ± 0.36 L/min vs healthy = 5.71 ± 0.32 L/min, <i>P</i> = .03) and SV (CF = 54 ± 5.5 mL/beat vs healthy = 73.3 ± 4.5 mL/beat, <i>P</i> = .01), and a higher HR (CF = 93.2 ± 3.9 bpm vs healthy = 80.5 ± 2.7 bpm, <i>P</i> < .01) and SVR (CF = 2082 ± 156 dynes*s/cm<sup>-5</sup> vs healthy = 1616 ± 74 dynes*s/cm<sup>-5</sup>, <i>P</i> = .01) compared with healthy subjects. Furthermore, CF patients demonstrated a lower SV (<i>P</i> < .01) corrected for NE when compared with healthy subjects. No significant differences were seen in HR or Q relative to NE, or SVR relative to EPI. Differences were seen in SV (F<sub>(2,14)</sub> = 7.982, <i>P</i> < .01) and SV index (F<sub>(2,14)</sub> = 2.913, <i>P</i> = .08) when patients with CF were stratified according to F508del mutation (number of deletions).</p><p><strong>Conclusions: </strong>Individuals with CF have lower cardiac and peripheral hemodynamic function parameters at rest. Furthermore, these results suggest that impairment in cardiovascular function is likely the result of F508del CFTR genotype, rather than receptor desensitization or inhibited drug delivery.</p>\",\"PeriodicalId\":44269,\"journal\":{\"name\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"volume\":\"13 \",\"pages\":\"1179548419835788\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2019-03-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179548419835788\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179548419835788\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179548419835788","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 5
摘要
背景:囊性纤维化(CF)是一种影响人体多器官系统的遗传性疾病,其特征是囊性纤维化跨膜传导调节因子(CFTR)基因编码突变。先前的研究表明,在健康受试者中,单剂量的aβ激动剂可增加心输出量(Q)和脑卒中量(SV),并降低全身血管阻力(SVR)。这种效应在CF患者中减弱;然而,其机制尚不清楚。CF患者对β-激动剂的心血管反应降低的潜在解释包括CFTR突变引起的固有心血管缺陷,长期使用β-激动剂作为临床护理的一部分导致受体脱敏,或由于肺部粘液积聚而抑制药物向血液的输送。本研究旨在确定内源性肾上腺素(EPI)和去甲肾上腺素(NE)对CF患者心血管功能的影响,并评估CFTR F508del突变与心血管功能的关系。方法:19例CF患者和31例健康对照者分别完成静止时Q (C2H2再呼吸)、SV(由Q和心率[HR]计算)、Q和SV与体表面积(分别为BSA、QI和SVI)、SVR(通过Q和平均动脉血压[MAP]评估)和HR(12导联心电图[ECG])的评估,并测量血浆EPI和NE。我们通过与EPI和NE相关的心血管功能变量,以及F508del突变的遗传变异(F508del纯合缺失、F508del杂合缺失或F508del无缺失)对受试者进行了比较。结果:囊性纤维化患者BSA (CF = 1.71±0.05 m2 vs健康者= 1.84±0.04 m2, P = 0.03)和SVI (CF = 30.6±2.5 mL/beat/m2 vs健康者= 39.9±2.5 mL/beat/m2, P = 0.02)显著低于健康者。囊性纤维化患者还演示了低Q (CF = 4.58±0.36 L / min vs健康= 5.71±0.32 L / min, P = 03)和SV (CF = 54±5.5 mL /击败vs健康= 73.3±4.5毫升/打,P = . 01),和更高的人力资源(CF bpm vs健康= 80.5 = 93.2±3.9±2.7 bpm, P < . 01)和SVR (CF = 2082±156达因* s / cm-5 vs健康= 1616±74达因* s / cm-5, P = . 01)与健康受试者相比。此外,与健康受试者相比,CF患者经NE校正后的SV更低(P < 0.01)。HR或Q相对于NE, SVR相对于EPI无显著差异。CF患者按F508del突变(缺失数)分层时,SV (F(2,14) = 7.982, P < 0.01)和SV指数(F(2,14) = 2.913, P = 0.08)有差异。结论:CF患者静息时心脏和外周血流动力学参数较低。此外,这些结果表明心血管功能的损害可能是F508del CFTR基因型的结果,而不是受体脱敏或抑制药物传递的结果。
Cystic Fibrosis Transmembrane Conductance Regulator Genotype, Not Circulating Catecholamines, Influences Cardiovascular Function in Patients with Cystic Fibrosis.
Background: Cystic fibrosis (CF) is a genetic disease affecting multiple organ systems of the body and is characterized by mutation in the gene coding for the cystic fibrosis transmembrane conductance regulator (CFTR). Previous work has shown that a single dose of aβ-agonist increases cardiac output (Q) and stroke volume (SV) and decreases systemic vascular resistance (SVR) in healthy subjects. This effect is attenuated in patients with CF; however, the mechanism is unknown. Potential explanations for this decreased cardiovascular response to a β-agonist in CF include inherent cardiovascular deficits secondary to the CFTR mutation, receptor desensitization from prolonged β-agonist use as part of clinical care, or inhibited drug delivery to the bloodstream due to mucus buildup in the lungs. This study sought to determine the effects of endogenous epinephrine (EPI) and norepinephrine (NE) on cardiovascular function in CF and to evaluate the relationship between cardiovascular function and CFTR F508del mutation.
Methods: A total of 19 patients with CF and 31 healthy control subjects completed an assessment of Q (C2H2 rebreathing), SV (calculated from Q and heart rate [HR]), Q and SV indexed to body surface area (BSA, QI, and SVI, respectively), SVR (through assessment of Q and mean arterial blood pressure [MAP]), and HR (from 12-lead electrocardiogram [ECG]) at rest along with plasma measures of EPI and NE. We compared subjects by variables of cardiovascular function relative to EPI and NE, and also based on genetic variants of the F508del mutation (homozygous deletion for F508del, heterozygous deletion for F508del, or no deletion of F508del).
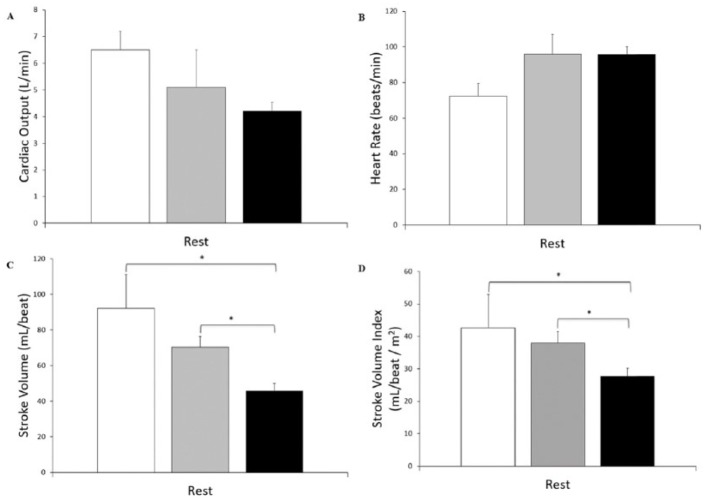
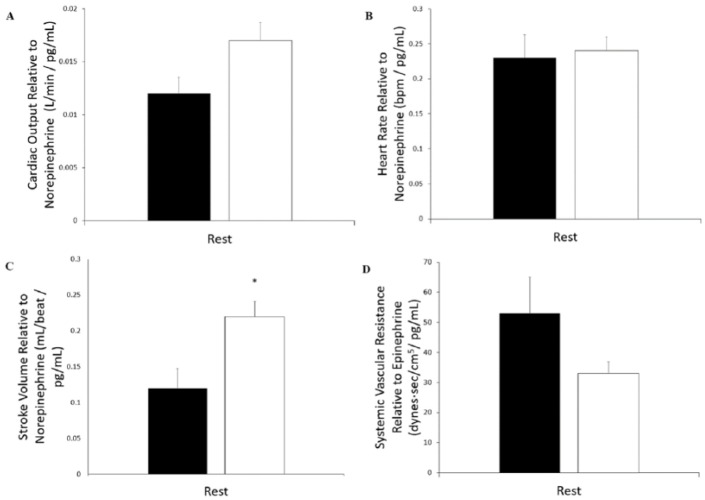
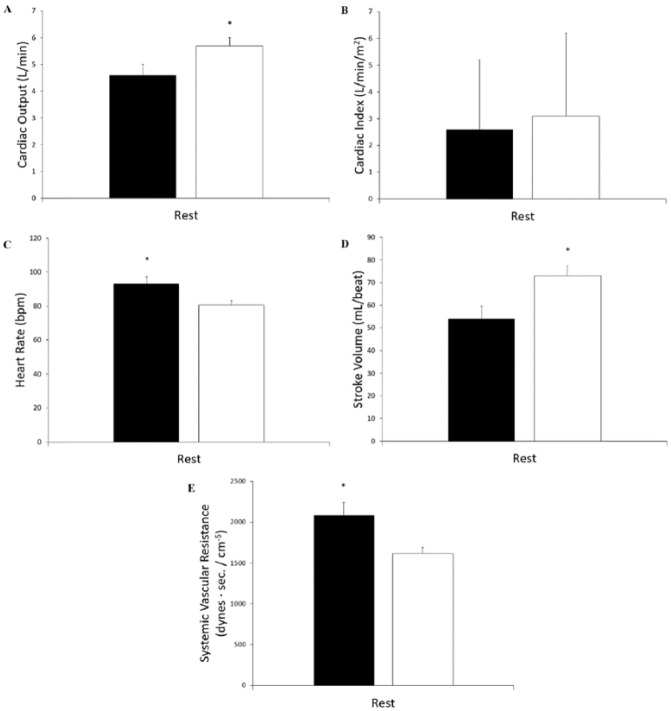
Results: Cystic fibrosis patients demonstrated significantly lower BSA (CF = 1.71 ± 0.05 m2 vs healthy = 1.84 ± 0.04 m2, P = .03) and SVI (CF = 30.6 ± 2.5 mL/beat/m2 vs healthy = 39.9 ± 2.5 mL/beat/m2, P = .02) when compared with healthy subjects. Cystic fibrosis patients also demonstrated lower Q (CF = 4.58 ± 0.36 L/min vs healthy = 5.71 ± 0.32 L/min, P = .03) and SV (CF = 54 ± 5.5 mL/beat vs healthy = 73.3 ± 4.5 mL/beat, P = .01), and a higher HR (CF = 93.2 ± 3.9 bpm vs healthy = 80.5 ± 2.7 bpm, P < .01) and SVR (CF = 2082 ± 156 dynes*s/cm-5 vs healthy = 1616 ± 74 dynes*s/cm-5, P = .01) compared with healthy subjects. Furthermore, CF patients demonstrated a lower SV (P < .01) corrected for NE when compared with healthy subjects. No significant differences were seen in HR or Q relative to NE, or SVR relative to EPI. Differences were seen in SV (F(2,14) = 7.982, P < .01) and SV index (F(2,14) = 2.913, P = .08) when patients with CF were stratified according to F508del mutation (number of deletions).
Conclusions: Individuals with CF have lower cardiac and peripheral hemodynamic function parameters at rest. Furthermore, these results suggest that impairment in cardiovascular function is likely the result of F508del CFTR genotype, rather than receptor desensitization or inhibited drug delivery.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
