Vasileios Kouritas, Richard Milton, Emmanouel Kefaloyannis, Kostas Papagiannopoulos, Allesandro Brunelli, Doytchin Dimov, Sishik Karthik, Andrew Hardy, Peter Tcherveniakov, Nilanjan Chaudhuri
{"title":"新成立的多学科团队对肺气肿患者介入治疗的影响。","authors":"Vasileios Kouritas, Richard Milton, Emmanouel Kefaloyannis, Kostas Papagiannopoulos, Allesandro Brunelli, Doytchin Dimov, Sishik Karthik, Andrew Hardy, Peter Tcherveniakov, Nilanjan Chaudhuri","doi":"10.1177/1179548419852063","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The emphysema interventional treatment involves mainly lung volume reduction surgery (LVRS) and endobronchial valve (EBV) implantation. Few institutes discuss these cases at a dedicated emphysema multidisciplinary team (MDT) meeting.</p><p><strong>Objectives: </strong>To investigate the impact of a newly established dedicated emphysema MDT meeting on the interventional treatment of such patients.</p><p><strong>Methods: </strong>During a study period of 4 years, the outcome of 44 patients who underwent intervention according to the proposal of the emphysema MDT (group A) was compared with the outcome of 44 propensity score matched patients (group B) treated without the emphysema MDT proposal.</p><p><strong>Results: </strong>More LVRS and less EBV insertions were performed in group A (<i>P </i>=<i> </i>.009). In group B, the interventions were performed sooner than in group A (<i>P </i>=<i> </i>.003). Postoperative overall morbidity and length of in-hospital stay were similar in the 2 groups (<i>P </i>=<i> </i>.918 and .758, respectively). Improvement of breathing ability was reported in more patients from group A (<i>P </i>=<i> </i>.012). In group B, the total number of re-interventions was higher (<i>P </i>=<i> </i>.001) and the time to re-intervention had the tendency to be less (<i>P </i>=<i> </i>.069). Survival was similar between the 2 groups (<i>P </i>=<i> </i>.884). Intervention without discussion at the MDT and EBV as initial intervention was an independent predictor of re-intervention.</p><p><strong>Conclusions: </strong>Interventional treatment for patients with chronic obstructive pulmonary disease (COPD) after discussion at a dedicated MDT involved more LVRS performed, required fewer interventions for their disease, and had longer re-intervention-free intervals and better breathing improvement.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"13 ","pages":"1179548419852063"},"PeriodicalIF":0.9000,"publicationDate":"2019-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179548419852063","citationCount":"4","resultStr":"{\"title\":\"The Impact of a Newly Established Multidisciplinary Team on the Interventional Treatment of Patients With Emphysema.\",\"authors\":\"Vasileios Kouritas, Richard Milton, Emmanouel Kefaloyannis, Kostas Papagiannopoulos, Allesandro Brunelli, Doytchin Dimov, Sishik Karthik, Andrew Hardy, Peter Tcherveniakov, Nilanjan Chaudhuri\",\"doi\":\"10.1177/1179548419852063\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The emphysema interventional treatment involves mainly lung volume reduction surgery (LVRS) and endobronchial valve (EBV) implantation. Few institutes discuss these cases at a dedicated emphysema multidisciplinary team (MDT) meeting.</p><p><strong>Objectives: </strong>To investigate the impact of a newly established dedicated emphysema MDT meeting on the interventional treatment of such patients.</p><p><strong>Methods: </strong>During a study period of 4 years, the outcome of 44 patients who underwent intervention according to the proposal of the emphysema MDT (group A) was compared with the outcome of 44 propensity score matched patients (group B) treated without the emphysema MDT proposal.</p><p><strong>Results: </strong>More LVRS and less EBV insertions were performed in group A (<i>P </i>=<i> </i>.009). In group B, the interventions were performed sooner than in group A (<i>P </i>=<i> </i>.003). Postoperative overall morbidity and length of in-hospital stay were similar in the 2 groups (<i>P </i>=<i> </i>.918 and .758, respectively). Improvement of breathing ability was reported in more patients from group A (<i>P </i>=<i> </i>.012). In group B, the total number of re-interventions was higher (<i>P </i>=<i> </i>.001) and the time to re-intervention had the tendency to be less (<i>P </i>=<i> </i>.069). Survival was similar between the 2 groups (<i>P </i>=<i> </i>.884). Intervention without discussion at the MDT and EBV as initial intervention was an independent predictor of re-intervention.</p><p><strong>Conclusions: </strong>Interventional treatment for patients with chronic obstructive pulmonary disease (COPD) after discussion at a dedicated MDT involved more LVRS performed, required fewer interventions for their disease, and had longer re-intervention-free intervals and better breathing improvement.</p>\",\"PeriodicalId\":44269,\"journal\":{\"name\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"volume\":\"13 \",\"pages\":\"1179548419852063\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2019-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179548419852063\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179548419852063\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179548419852063","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
The Impact of a Newly Established Multidisciplinary Team on the Interventional Treatment of Patients With Emphysema.
Background: The emphysema interventional treatment involves mainly lung volume reduction surgery (LVRS) and endobronchial valve (EBV) implantation. Few institutes discuss these cases at a dedicated emphysema multidisciplinary team (MDT) meeting.
Objectives: To investigate the impact of a newly established dedicated emphysema MDT meeting on the interventional treatment of such patients.
Methods: During a study period of 4 years, the outcome of 44 patients who underwent intervention according to the proposal of the emphysema MDT (group A) was compared with the outcome of 44 propensity score matched patients (group B) treated without the emphysema MDT proposal.
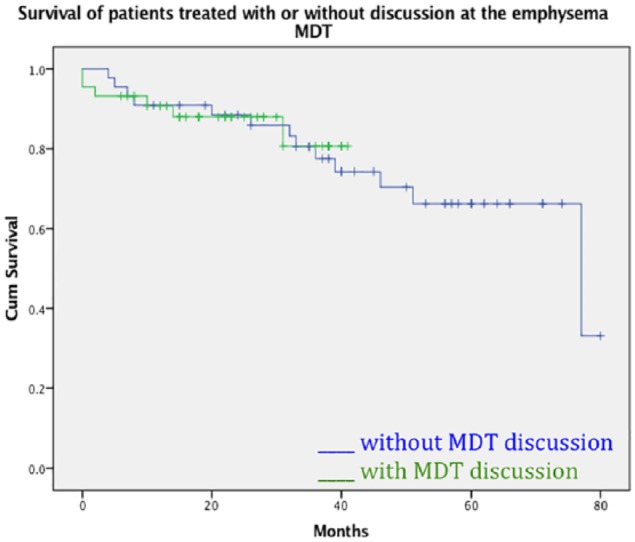
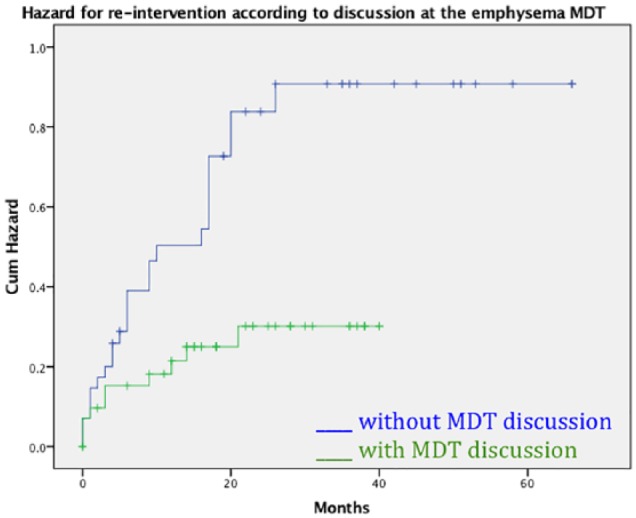
Results: More LVRS and less EBV insertions were performed in group A (P =.009). In group B, the interventions were performed sooner than in group A (P =.003). Postoperative overall morbidity and length of in-hospital stay were similar in the 2 groups (P =.918 and .758, respectively). Improvement of breathing ability was reported in more patients from group A (P =.012). In group B, the total number of re-interventions was higher (P =.001) and the time to re-intervention had the tendency to be less (P =.069). Survival was similar between the 2 groups (P =.884). Intervention without discussion at the MDT and EBV as initial intervention was an independent predictor of re-intervention.
Conclusions: Interventional treatment for patients with chronic obstructive pulmonary disease (COPD) after discussion at a dedicated MDT involved more LVRS performed, required fewer interventions for their disease, and had longer re-intervention-free intervals and better breathing improvement.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
