{"title":"心肌梗死左心室游离壁破裂:来自单一三级中心的回顾性分析。","authors":"Swaroop Varghese, Marc-Alexander Ohlow","doi":"10.1177/2048004019896692","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Left ventricular free wall rupture (LVFWR) is a rare but severe complication of acute myocardial infarction (AMI). During the era of pre-thrombolysis, autopsies revealed an incidence of approximately 8%.</p><p><strong>Method: </strong>The objective of this retrospective study was to analyze the current incidence of LVFWR and to identify predictors by comparing the AMI-cohort with LVFWR to those without. The control group involved a random selection of one in every ten patients who presented with acute myocardial infarction between 2005 and 2014.</p><p><strong>Result: </strong>A total of 5143 patients with AMI were treated at the Central Hospital, Bad Berka (71% men, median age 68 years). Out of these, seven patients with LVFWR were identified with an overall incidence of 0.14%. Clinically, LVFWR patients presented late to admission since symptom onset (median 24 h vs. 6.1 h; p < 0.0001), were more likely in cardiogenic shock (28.6% vs. 3.2%; p = 0.02) and were usually accompanied by emergency physicians (71.4% vs. 20.7%; p = 0.006). Higher troponin T (median 8.6 vs. 0.5 ng/ml; p < 0.0002), higher CRP (median 50 vs. 0.5 mg/l; p = 0.05) as well as a lower hematocrit-values (0.33 vs. 0.42; p = 0.04) were observed. All LVFWR patients were operated (100% vs. 1.6%; p < 0.001). The patients had lower rates of beta-blocker treatment (57.1% vs. 95.8%; p = 0.003). The 30-day mortality was significantly higher (42.9% vs. 6.8%; p = 0.01).</p><p><strong>Conclusion: </strong>Compared to the thrombolytic era, the current incidence of LVFWR with AMI, who reach the hospital alive, is significantly lower. However, 30-day mortality continues to be high.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"8 ","pages":"2048004019896692"},"PeriodicalIF":0.6000,"publicationDate":"2019-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2048004019896692","citationCount":"11","resultStr":"{\"title\":\"Left ventricular free wall rupture in myocardial infarction: A retrospective analysis from a single tertiary center.\",\"authors\":\"Swaroop Varghese, Marc-Alexander Ohlow\",\"doi\":\"10.1177/2048004019896692\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Left ventricular free wall rupture (LVFWR) is a rare but severe complication of acute myocardial infarction (AMI). During the era of pre-thrombolysis, autopsies revealed an incidence of approximately 8%.</p><p><strong>Method: </strong>The objective of this retrospective study was to analyze the current incidence of LVFWR and to identify predictors by comparing the AMI-cohort with LVFWR to those without. The control group involved a random selection of one in every ten patients who presented with acute myocardial infarction between 2005 and 2014.</p><p><strong>Result: </strong>A total of 5143 patients with AMI were treated at the Central Hospital, Bad Berka (71% men, median age 68 years). Out of these, seven patients with LVFWR were identified with an overall incidence of 0.14%. Clinically, LVFWR patients presented late to admission since symptom onset (median 24 h vs. 6.1 h; p < 0.0001), were more likely in cardiogenic shock (28.6% vs. 3.2%; p = 0.02) and were usually accompanied by emergency physicians (71.4% vs. 20.7%; p = 0.006). Higher troponin T (median 8.6 vs. 0.5 ng/ml; p < 0.0002), higher CRP (median 50 vs. 0.5 mg/l; p = 0.05) as well as a lower hematocrit-values (0.33 vs. 0.42; p = 0.04) were observed. All LVFWR patients were operated (100% vs. 1.6%; p < 0.001). The patients had lower rates of beta-blocker treatment (57.1% vs. 95.8%; p = 0.003). The 30-day mortality was significantly higher (42.9% vs. 6.8%; p = 0.01).</p><p><strong>Conclusion: </strong>Compared to the thrombolytic era, the current incidence of LVFWR with AMI, who reach the hospital alive, is significantly lower. However, 30-day mortality continues to be high.</p>\",\"PeriodicalId\":30457,\"journal\":{\"name\":\"JRSM Cardiovascular Disease\",\"volume\":\"8 \",\"pages\":\"2048004019896692\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2019-12-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/2048004019896692\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JRSM Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2048004019896692\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2048004019896692","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Left ventricular free wall rupture in myocardial infarction: A retrospective analysis from a single tertiary center.
Objective: Left ventricular free wall rupture (LVFWR) is a rare but severe complication of acute myocardial infarction (AMI). During the era of pre-thrombolysis, autopsies revealed an incidence of approximately 8%.
Method: The objective of this retrospective study was to analyze the current incidence of LVFWR and to identify predictors by comparing the AMI-cohort with LVFWR to those without. The control group involved a random selection of one in every ten patients who presented with acute myocardial infarction between 2005 and 2014.
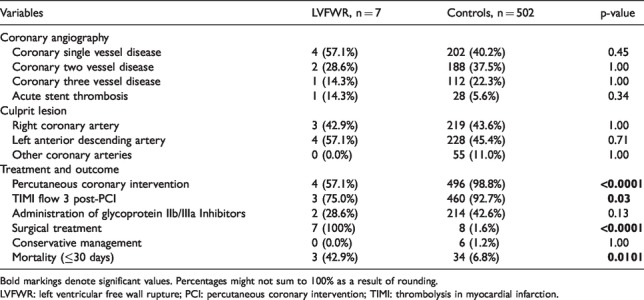
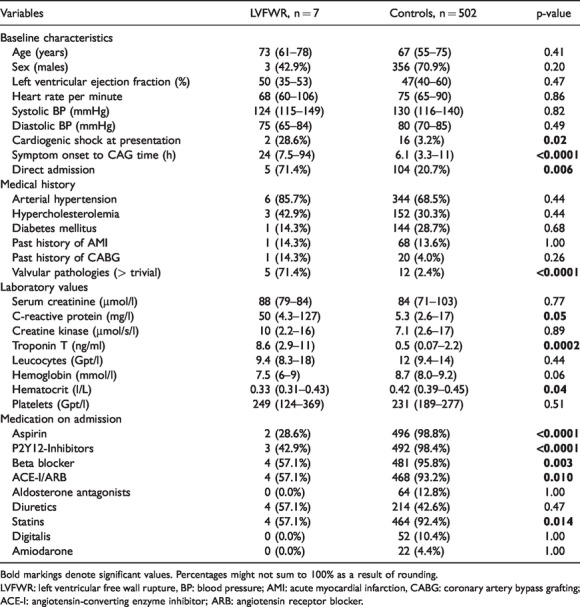
Result: A total of 5143 patients with AMI were treated at the Central Hospital, Bad Berka (71% men, median age 68 years). Out of these, seven patients with LVFWR were identified with an overall incidence of 0.14%. Clinically, LVFWR patients presented late to admission since symptom onset (median 24 h vs. 6.1 h; p < 0.0001), were more likely in cardiogenic shock (28.6% vs. 3.2%; p = 0.02) and were usually accompanied by emergency physicians (71.4% vs. 20.7%; p = 0.006). Higher troponin T (median 8.6 vs. 0.5 ng/ml; p < 0.0002), higher CRP (median 50 vs. 0.5 mg/l; p = 0.05) as well as a lower hematocrit-values (0.33 vs. 0.42; p = 0.04) were observed. All LVFWR patients were operated (100% vs. 1.6%; p < 0.001). The patients had lower rates of beta-blocker treatment (57.1% vs. 95.8%; p = 0.003). The 30-day mortality was significantly higher (42.9% vs. 6.8%; p = 0.01).
Conclusion: Compared to the thrombolytic era, the current incidence of LVFWR with AMI, who reach the hospital alive, is significantly lower. However, 30-day mortality continues to be high.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
