Angelina Grest, Judith Kurmann, Markus Müller, Victor Jeger, Bernard Krüger, Donat R Spahn, Dominique Bettex, Alain Rudiger
{"title":"可乐定和右美托咪定在危重患者心脏手术后心血管的安全性。","authors":"Angelina Grest, Judith Kurmann, Markus Müller, Victor Jeger, Bernard Krüger, Donat R Spahn, Dominique Bettex, Alain Rudiger","doi":"10.1155/2020/4750615","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The aim of this retrospective study was to assess the haemodynamic adverse effects of clonidine and dexmedetomidine in critically ill patients after cardiac surgery.</p><p><strong>Methods: </strong>2769 patients were screened during the 30-month study period. Heart rate (HR), mean arterial pressure (MAP), and norepinephrine requirements were assessed 3-hourly during the first 12 hours of the continuous drug infusion. Results are given as median (interquartile range) or numbers (percentages).</p><p><strong>Results: </strong>Patients receiving clonidine (<i>n</i> = 193) were younger (66 (57-73) vs 70 (63-77) years, <i>p</i>=0.003) and had a lower SAPS II (35 (27-48) vs 41 (31-54), <i>p</i>=0.008) compared with patients receiving dexmedetomidine (<i>n</i> = 141). At the start of the drug infusion, HR (90 (75-100) vs 90 (80-105) bpm, <i>p</i>=0.028), MAP (70 (65-80) vs 70 (65-75) mmHg, <i>p</i>=0.093), and norepinephrine (0.05 (0.00-0.11) vs 0.12 (0.03-0.19) mcg/kg/min, <i>p</i> < 0.001) were recorded in patients with clonidine and dexmedetomidine. Bradycardia (HR < 60 bpm) developed in 7.8% with clonidine and 5.7% with dexmedetomidine (<i>p</i>=0.51). Between baseline and 12 hours, norepinephrine remained stable in the clonidine group (0.00 (-0.04-0.02) mcg/kg/min) and decreased in the dexmedetomidine group (-0.03 (-0.10-0.02) mcg/kg/min, <i>p</i>=0.007).</p><p><strong>Conclusions: </strong>Dexmedetomidine and the low-cost drug clonidine can both be used safely in selected patients after cardiac surgery.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2020 ","pages":"4750615"},"PeriodicalIF":1.8000,"publicationDate":"2020-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/4750615","citationCount":"3","resultStr":"{\"title\":\"Cardiovascular Safety of Clonidine and Dexmedetomidine in Critically Ill Patients after Cardiac Surgery.\",\"authors\":\"Angelina Grest, Judith Kurmann, Markus Müller, Victor Jeger, Bernard Krüger, Donat R Spahn, Dominique Bettex, Alain Rudiger\",\"doi\":\"10.1155/2020/4750615\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The aim of this retrospective study was to assess the haemodynamic adverse effects of clonidine and dexmedetomidine in critically ill patients after cardiac surgery.</p><p><strong>Methods: </strong>2769 patients were screened during the 30-month study period. Heart rate (HR), mean arterial pressure (MAP), and norepinephrine requirements were assessed 3-hourly during the first 12 hours of the continuous drug infusion. Results are given as median (interquartile range) or numbers (percentages).</p><p><strong>Results: </strong>Patients receiving clonidine (<i>n</i> = 193) were younger (66 (57-73) vs 70 (63-77) years, <i>p</i>=0.003) and had a lower SAPS II (35 (27-48) vs 41 (31-54), <i>p</i>=0.008) compared with patients receiving dexmedetomidine (<i>n</i> = 141). At the start of the drug infusion, HR (90 (75-100) vs 90 (80-105) bpm, <i>p</i>=0.028), MAP (70 (65-80) vs 70 (65-75) mmHg, <i>p</i>=0.093), and norepinephrine (0.05 (0.00-0.11) vs 0.12 (0.03-0.19) mcg/kg/min, <i>p</i> < 0.001) were recorded in patients with clonidine and dexmedetomidine. Bradycardia (HR < 60 bpm) developed in 7.8% with clonidine and 5.7% with dexmedetomidine (<i>p</i>=0.51). Between baseline and 12 hours, norepinephrine remained stable in the clonidine group (0.00 (-0.04-0.02) mcg/kg/min) and decreased in the dexmedetomidine group (-0.03 (-0.10-0.02) mcg/kg/min, <i>p</i>=0.007).</p><p><strong>Conclusions: </strong>Dexmedetomidine and the low-cost drug clonidine can both be used safely in selected patients after cardiac surgery.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2020 \",\"pages\":\"4750615\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/4750615\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/4750615\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/4750615","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 3
摘要
目的:本回顾性研究的目的是评估可乐定和右美托咪定对心脏手术后危重患者血流动力学的不良影响。方法:在30个月的研究期间筛选2769例患者。心率(HR)、平均动脉压(MAP)和去甲肾上腺素需要量在连续输注药物的前12小时内每3小时进行评估。结果以中位数(四分位数范围)或数字(百分比)给出。结果:接受可乐定治疗的患者(n = 193)比接受右美托咪定治疗的患者(n = 141)更年轻(66 (57-73)vs 70 (63-77), p=0.003), SAPS II (35 (27-48) vs 41 (31-54), p=0.008)。在药物输注开始时,记录下可乐定和右美托咪定患者的HR (90 (75-100) vs 90 (80-105) bpm, p=0.028)、MAP (70 (65-80) vs 70 (65-75) mmHg, p=0.093)和去甲肾上腺素(0.05 (0.00-0.11)vs 0.12 (0.03-0.19) mcg/kg/min, p < 0.001)。心动过缓(HR p=0.51)。从基线到12小时,可乐定组的去甲肾上腺素保持稳定(0.00 (-0.04-0.02)mcg/kg/min),右美托咪定组的去甲肾上腺素下降(-0.03 (-0.10-0.02)mcg/kg/min, p=0.007)。结论:右美托咪定与低成本药物可乐定均可安全用于选定的心脏术后患者。
Cardiovascular Safety of Clonidine and Dexmedetomidine in Critically Ill Patients after Cardiac Surgery.
Purpose: The aim of this retrospective study was to assess the haemodynamic adverse effects of clonidine and dexmedetomidine in critically ill patients after cardiac surgery.
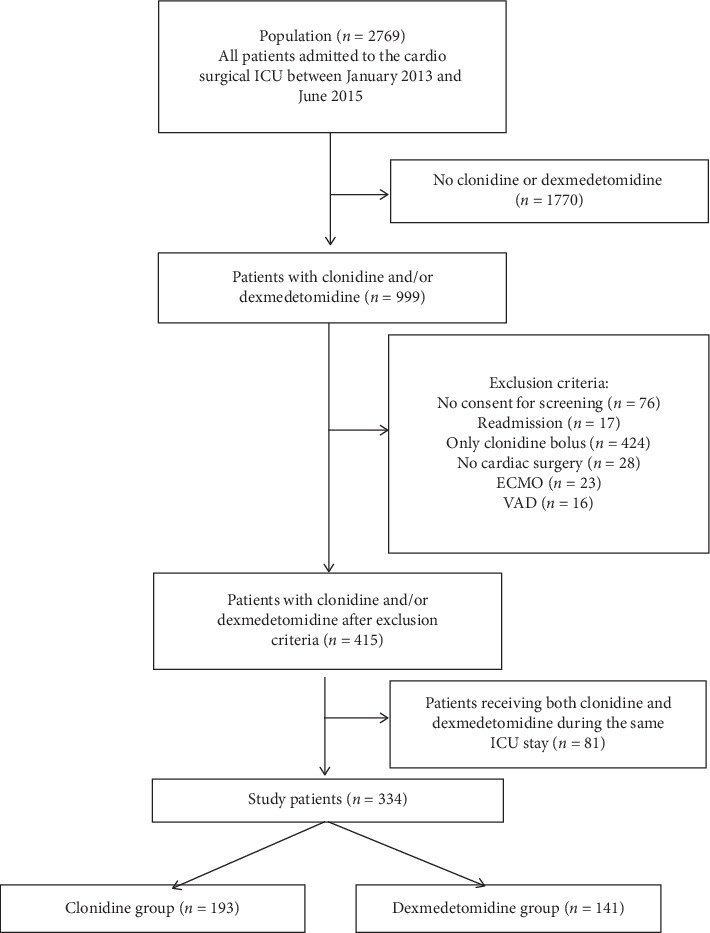
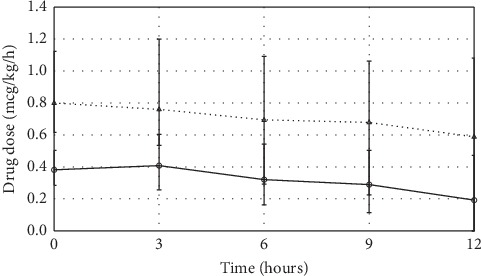
Methods: 2769 patients were screened during the 30-month study period. Heart rate (HR), mean arterial pressure (MAP), and norepinephrine requirements were assessed 3-hourly during the first 12 hours of the continuous drug infusion. Results are given as median (interquartile range) or numbers (percentages).
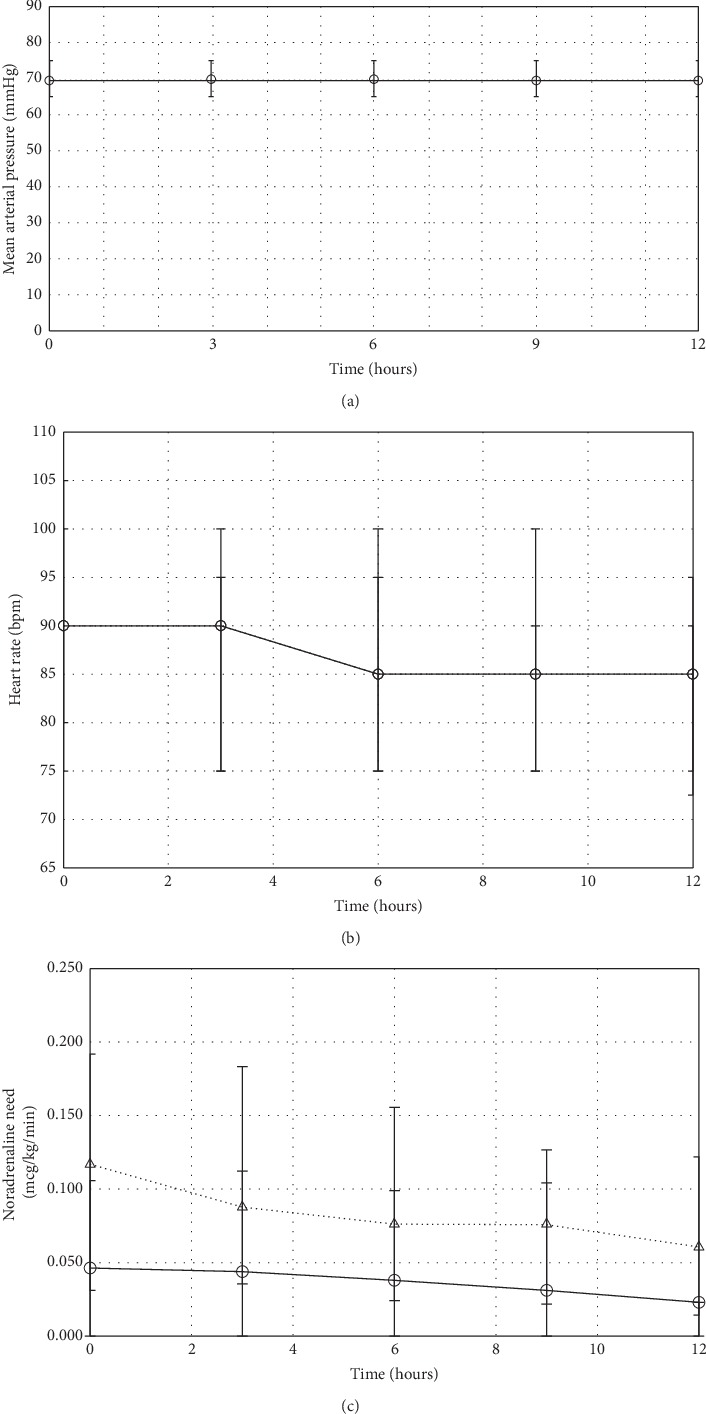
Results: Patients receiving clonidine (n = 193) were younger (66 (57-73) vs 70 (63-77) years, p=0.003) and had a lower SAPS II (35 (27-48) vs 41 (31-54), p=0.008) compared with patients receiving dexmedetomidine (n = 141). At the start of the drug infusion, HR (90 (75-100) vs 90 (80-105) bpm, p=0.028), MAP (70 (65-80) vs 70 (65-75) mmHg, p=0.093), and norepinephrine (0.05 (0.00-0.11) vs 0.12 (0.03-0.19) mcg/kg/min, p < 0.001) were recorded in patients with clonidine and dexmedetomidine. Bradycardia (HR < 60 bpm) developed in 7.8% with clonidine and 5.7% with dexmedetomidine (p=0.51). Between baseline and 12 hours, norepinephrine remained stable in the clonidine group (0.00 (-0.04-0.02) mcg/kg/min) and decreased in the dexmedetomidine group (-0.03 (-0.10-0.02) mcg/kg/min, p=0.007).
Conclusions: Dexmedetomidine and the low-cost drug clonidine can both be used safely in selected patients after cardiac surgery.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
