{"title":"进行性家族性2型肝内胆汁淤积症双胞胎佝偻病和血脂异常的治疗。","authors":"Sunitha R Sura, Emily L Germain-Lee","doi":"10.1186/s13633-020-00079-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Progressive Familial Intrahepatic Cholestasis Type 2 (PFIC2) is a rare congenital cholestatic liver disease that progresses to end stage liver disease. It is associated with fat soluble vitamin D deficiency rickets and severe dyslipidemia; however, treatment of these secondary effects remains a challenge.</p><p><strong>Case presentation: </strong>One year old twin males born to a mother with intrahepatic cholestasis during pregnancy presented with jaundice, pruritus and failure to thrive. Lab evaluation revealed significant transaminitis, direct hyperbilirubinemia and normal gamma glutamyl transferase (GGT). Genetic studies confirmed PFIC2. Further evaluation for fat soluble vitamin deficiencies revealed severe vitamin D deficiency rickets. High dose vitamin D replacement therapy using Ergocalciferol (Vitamin D<sub>2</sub>) 50,000 IU three times a week over 10 weeks led to the improvement of Vitamin D, 25-Hydroxy (25-OH) serum levels and resolution of rickets. Dyslipidemia with very low high density lipoprotein-cholesterol (HDL-C) and high triglycerides was more profound in our patients compared to what has been described in the literature thus far. The dyslipidemia improved 2 months after internal biliary diversion.</p><p><strong>Conclusions: </strong>Higher doses of Vitamin D therapy are needed for treatment of rickets secondary to cholestasis. Extremely low HDL-C levels are characteristic of PFIC and improve with treatment of underlying cholestasis. Maternal intrahepatic cholestasis during pregnancy can be an early warning sign.</p>","PeriodicalId":14271,"journal":{"name":"International Journal of Pediatric Endocrinology","volume":"2020 ","pages":"9"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13633-020-00079-1","citationCount":"1","resultStr":"{\"title\":\"Treatment of rickets and dyslipidemia in twins with progressive familial intrahepatic cholestasis type 2.\",\"authors\":\"Sunitha R Sura, Emily L Germain-Lee\",\"doi\":\"10.1186/s13633-020-00079-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Progressive Familial Intrahepatic Cholestasis Type 2 (PFIC2) is a rare congenital cholestatic liver disease that progresses to end stage liver disease. It is associated with fat soluble vitamin D deficiency rickets and severe dyslipidemia; however, treatment of these secondary effects remains a challenge.</p><p><strong>Case presentation: </strong>One year old twin males born to a mother with intrahepatic cholestasis during pregnancy presented with jaundice, pruritus and failure to thrive. Lab evaluation revealed significant transaminitis, direct hyperbilirubinemia and normal gamma glutamyl transferase (GGT). Genetic studies confirmed PFIC2. Further evaluation for fat soluble vitamin deficiencies revealed severe vitamin D deficiency rickets. High dose vitamin D replacement therapy using Ergocalciferol (Vitamin D<sub>2</sub>) 50,000 IU three times a week over 10 weeks led to the improvement of Vitamin D, 25-Hydroxy (25-OH) serum levels and resolution of rickets. Dyslipidemia with very low high density lipoprotein-cholesterol (HDL-C) and high triglycerides was more profound in our patients compared to what has been described in the literature thus far. The dyslipidemia improved 2 months after internal biliary diversion.</p><p><strong>Conclusions: </strong>Higher doses of Vitamin D therapy are needed for treatment of rickets secondary to cholestasis. Extremely low HDL-C levels are characteristic of PFIC and improve with treatment of underlying cholestasis. Maternal intrahepatic cholestasis during pregnancy can be an early warning sign.</p>\",\"PeriodicalId\":14271,\"journal\":{\"name\":\"International Journal of Pediatric Endocrinology\",\"volume\":\"2020 \",\"pages\":\"9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13633-020-00079-1\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Pediatric Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13633-020-00079-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/5/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13633-020-00079-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/5/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Treatment of rickets and dyslipidemia in twins with progressive familial intrahepatic cholestasis type 2.
Background: Progressive Familial Intrahepatic Cholestasis Type 2 (PFIC2) is a rare congenital cholestatic liver disease that progresses to end stage liver disease. It is associated with fat soluble vitamin D deficiency rickets and severe dyslipidemia; however, treatment of these secondary effects remains a challenge.
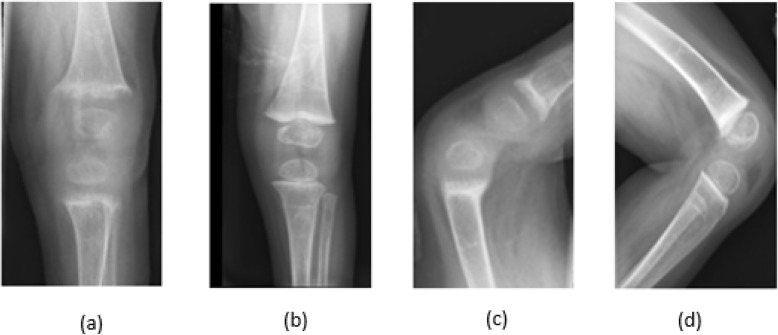
Case presentation: One year old twin males born to a mother with intrahepatic cholestasis during pregnancy presented with jaundice, pruritus and failure to thrive. Lab evaluation revealed significant transaminitis, direct hyperbilirubinemia and normal gamma glutamyl transferase (GGT). Genetic studies confirmed PFIC2. Further evaluation for fat soluble vitamin deficiencies revealed severe vitamin D deficiency rickets. High dose vitamin D replacement therapy using Ergocalciferol (Vitamin D2) 50,000 IU three times a week over 10 weeks led to the improvement of Vitamin D, 25-Hydroxy (25-OH) serum levels and resolution of rickets. Dyslipidemia with very low high density lipoprotein-cholesterol (HDL-C) and high triglycerides was more profound in our patients compared to what has been described in the literature thus far. The dyslipidemia improved 2 months after internal biliary diversion.
Conclusions: Higher doses of Vitamin D therapy are needed for treatment of rickets secondary to cholestasis. Extremely low HDL-C levels are characteristic of PFIC and improve with treatment of underlying cholestasis. Maternal intrahepatic cholestasis during pregnancy can be an early warning sign.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
