Aniket S Rali, Sergio Trevino, Edward Yang, James P Herlihy, Jose Diaz-Gomez
{"title":"重症冠状病毒病2019患者俯卧位心肺超声检查","authors":"Aniket S Rali, Sergio Trevino, Edward Yang, James P Herlihy, Jose Diaz-Gomez","doi":"10.15420/cfr.2020.12","DOIUrl":null,"url":null,"abstract":"Case Presentation A 50-year old female presented to the emergency department with a 6-day history of fever, progressively worsening cough and shortness of breath. The patient did not report any contact with anyone who had been recently unwell or had been travelling. Upon arrival to the emergency room, the patient was noted to be severely hypoxaemic by pulse oximetry (66%) and in impeding respiratory failure, so she was emergently intubated for mechanical ventilatory support. Immediately post-intubation, arterial blood gas was as follows: pH 7.34, pCO 2 31 mmHg, pO 2 60 mmHg, O 2 saturation 90%, calculated HCO 3 16 mmol/l on FiO 2 of 100% and PaO 2 /FIO 2 ratio of 60. Her ventilatory mode was set at controlled minute ventilation, with a respiratory rate of 24, tidal volume of 300 cc (6 cc/ ideal body weight), positive end-expiratory pressure (PEEP) of 20 cmH 2 O and FiO 2 of 100%. The patient’s chest X-ray at the time of admission showed diffuse bilateral pulmonary opacities consistent with multifocal pneumonia or pulmonary oedema (Figure 1). Polymerase chain reaction (PCR) testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was sent and came back positive after 48 hours.","PeriodicalId":33741,"journal":{"name":"Cardiac Failure Review","volume":"6 ","pages":"e12"},"PeriodicalIF":5.7000,"publicationDate":"2020-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/0f/cfr-06-e12.PMC7265100.pdf","citationCount":"2","resultStr":"{\"title\":\"Cardiopulmonary Ultrasonography for Severe Coronavirus Disease 2019 Patients in Prone Position.\",\"authors\":\"Aniket S Rali, Sergio Trevino, Edward Yang, James P Herlihy, Jose Diaz-Gomez\",\"doi\":\"10.15420/cfr.2020.12\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Case Presentation A 50-year old female presented to the emergency department with a 6-day history of fever, progressively worsening cough and shortness of breath. The patient did not report any contact with anyone who had been recently unwell or had been travelling. Upon arrival to the emergency room, the patient was noted to be severely hypoxaemic by pulse oximetry (66%) and in impeding respiratory failure, so she was emergently intubated for mechanical ventilatory support. Immediately post-intubation, arterial blood gas was as follows: pH 7.34, pCO 2 31 mmHg, pO 2 60 mmHg, O 2 saturation 90%, calculated HCO 3 16 mmol/l on FiO 2 of 100% and PaO 2 /FIO 2 ratio of 60. Her ventilatory mode was set at controlled minute ventilation, with a respiratory rate of 24, tidal volume of 300 cc (6 cc/ ideal body weight), positive end-expiratory pressure (PEEP) of 20 cmH 2 O and FiO 2 of 100%. The patient’s chest X-ray at the time of admission showed diffuse bilateral pulmonary opacities consistent with multifocal pneumonia or pulmonary oedema (Figure 1). Polymerase chain reaction (PCR) testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was sent and came back positive after 48 hours.\",\"PeriodicalId\":33741,\"journal\":{\"name\":\"Cardiac Failure Review\",\"volume\":\"6 \",\"pages\":\"e12\"},\"PeriodicalIF\":5.7000,\"publicationDate\":\"2020-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/0f/cfr-06-e12.PMC7265100.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiac Failure Review\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15420/cfr.2020.12\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiac Failure Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/cfr.2020.12","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/3/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Cardiopulmonary Ultrasonography for Severe Coronavirus Disease 2019 Patients in Prone Position.
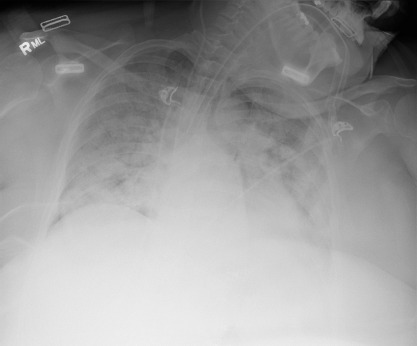
Case Presentation A 50-year old female presented to the emergency department with a 6-day history of fever, progressively worsening cough and shortness of breath. The patient did not report any contact with anyone who had been recently unwell or had been travelling. Upon arrival to the emergency room, the patient was noted to be severely hypoxaemic by pulse oximetry (66%) and in impeding respiratory failure, so she was emergently intubated for mechanical ventilatory support. Immediately post-intubation, arterial blood gas was as follows: pH 7.34, pCO 2 31 mmHg, pO 2 60 mmHg, O 2 saturation 90%, calculated HCO 3 16 mmol/l on FiO 2 of 100% and PaO 2 /FIO 2 ratio of 60. Her ventilatory mode was set at controlled minute ventilation, with a respiratory rate of 24, tidal volume of 300 cc (6 cc/ ideal body weight), positive end-expiratory pressure (PEEP) of 20 cmH 2 O and FiO 2 of 100%. The patient’s chest X-ray at the time of admission showed diffuse bilateral pulmonary opacities consistent with multifocal pneumonia or pulmonary oedema (Figure 1). Polymerase chain reaction (PCR) testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was sent and came back positive after 48 hours.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
