{"title":"危重病人心输出量的连续评估:一种基于脉搏波传递时间与经肺热调节的无创方法。","authors":"Ulrike Ehlers, Rolf Erlebach, Giovanna Brandi, Federica Stretti, Richard Valek, Stephanie Klinzing, Reto Schuepbach","doi":"10.1155/2020/8956372","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Estimation of cardiac output (CO) and evaluation of change in CO as a result of therapeutic interventions are essential in critical care medicine. Whether noninvasive tools estimating CO, such as continuous cardiac output (esCCOTM) methods, are sufficiently accurate and precise to guide therapy needs further evaluation. We compared esCCOTM with an established method, namely, transpulmonary thermodilution (TPTD). <i>Patients and Methods</i>. In a single center mixed ICU, esCCOTM was compared with the TPTD method in 38 patients. The primary endpoint was accuracy and precision. The cardiac output was assessed by two investigators at baseline and after eight hours.</p><p><strong>Results: </strong>In 38 critically ill patients, the two methods correlated significantly (<i>r</i> = 0.742). The Bland-Altman analysis showed a bias of 1.6 l/min with limits of agreement of -1.76 l/min and +4.98 l/min. The percentage error for CO<sub>esCCO</sub> was 47%. The correlation of trends in cardiac output after eight hours was significant (<i>r</i> = 0.442), with a concordance of 74%. The performance of CO<sub>esCCO</sub> could not be linked to the patient's condition.</p><p><strong>Conclusion: </strong>The accuracy and precision of the esCCOTM method were not clinically acceptable for our critical patients. EsCCOTM also failed to reliably detect changes in cardiac output.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2020 ","pages":"8956372"},"PeriodicalIF":1.8000,"publicationDate":"2020-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/8956372","citationCount":"2","resultStr":"{\"title\":\"Continuous Estimation of Cardiac Output in Critical Care: A Noninvasive Method Based on Pulse Wave Transit Time Compared with Transpulmonary Thermodilution.\",\"authors\":\"Ulrike Ehlers, Rolf Erlebach, Giovanna Brandi, Federica Stretti, Richard Valek, Stephanie Klinzing, Reto Schuepbach\",\"doi\":\"10.1155/2020/8956372\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Estimation of cardiac output (CO) and evaluation of change in CO as a result of therapeutic interventions are essential in critical care medicine. Whether noninvasive tools estimating CO, such as continuous cardiac output (esCCOTM) methods, are sufficiently accurate and precise to guide therapy needs further evaluation. We compared esCCOTM with an established method, namely, transpulmonary thermodilution (TPTD). <i>Patients and Methods</i>. In a single center mixed ICU, esCCOTM was compared with the TPTD method in 38 patients. The primary endpoint was accuracy and precision. The cardiac output was assessed by two investigators at baseline and after eight hours.</p><p><strong>Results: </strong>In 38 critically ill patients, the two methods correlated significantly (<i>r</i> = 0.742). The Bland-Altman analysis showed a bias of 1.6 l/min with limits of agreement of -1.76 l/min and +4.98 l/min. The percentage error for CO<sub>esCCO</sub> was 47%. The correlation of trends in cardiac output after eight hours was significant (<i>r</i> = 0.442), with a concordance of 74%. The performance of CO<sub>esCCO</sub> could not be linked to the patient's condition.</p><p><strong>Conclusion: </strong>The accuracy and precision of the esCCOTM method were not clinically acceptable for our critical patients. EsCCOTM also failed to reliably detect changes in cardiac output.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2020 \",\"pages\":\"8956372\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-07-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/8956372\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/8956372\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/8956372","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Continuous Estimation of Cardiac Output in Critical Care: A Noninvasive Method Based on Pulse Wave Transit Time Compared with Transpulmonary Thermodilution.
Purpose: Estimation of cardiac output (CO) and evaluation of change in CO as a result of therapeutic interventions are essential in critical care medicine. Whether noninvasive tools estimating CO, such as continuous cardiac output (esCCOTM) methods, are sufficiently accurate and precise to guide therapy needs further evaluation. We compared esCCOTM with an established method, namely, transpulmonary thermodilution (TPTD). Patients and Methods. In a single center mixed ICU, esCCOTM was compared with the TPTD method in 38 patients. The primary endpoint was accuracy and precision. The cardiac output was assessed by two investigators at baseline and after eight hours.
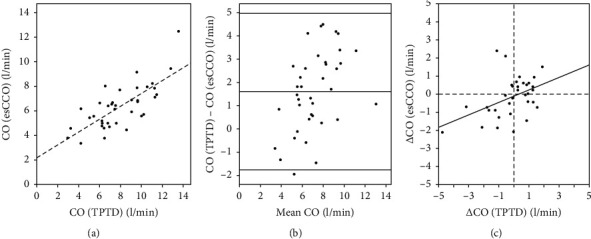
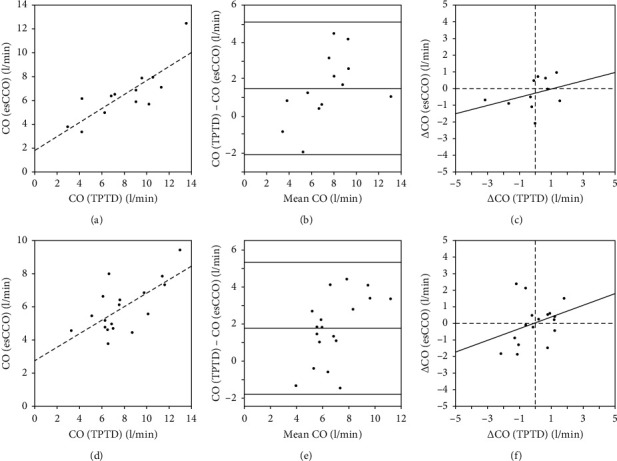
Results: In 38 critically ill patients, the two methods correlated significantly (r = 0.742). The Bland-Altman analysis showed a bias of 1.6 l/min with limits of agreement of -1.76 l/min and +4.98 l/min. The percentage error for COesCCO was 47%. The correlation of trends in cardiac output after eight hours was significant (r = 0.442), with a concordance of 74%. The performance of COesCCO could not be linked to the patient's condition.
Conclusion: The accuracy and precision of the esCCOTM method were not clinically acceptable for our critical patients. EsCCOTM also failed to reliably detect changes in cardiac output.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
