{"title":"造影剂诱导的急性肾损伤对心力衰竭患者肾素-血管紧张素系统抑制剂与长期死亡率之间关系的影响。","authors":"Li Lei, Yulu Huang, Zhaodong Guo, Feier Song, Yibo He, Jin Liu, Guoli Sun, Bowen Liu, Pengyuan Chen, Jianbin Zhao, Dengxuan Wu, Yan Xue, Wenhe Yan, Zefeng Lin, Xiuqiong Huang, Guanzhong Chen, Shiqun Chen, Yong Liu, Jiyan Chen","doi":"10.1177/1470320320979795","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Renin-angiotensin system inhibitors (RASi) reduce mortality among heart failure (HF) patients, but their effect among those complicating contrast-induced acute kidney injury (CI-AKI) remains unexplored. We aimed to investigate whether the relationship between RASi prescription at discharge and mortality differs between HF patients with or without CI-AKI following coronary angiography (CAG).</p><p><strong>Methods: </strong>About 596 HF patients from an observational cohort were divided into a CI-AKI group (<i>n</i> = 104) and a non-CI-AKI group (<i>n</i> = 492) based on whether they had CI-AKI following CAG. The endpoint was all-cause mortality. Multivariable Cox regression was performed in each group to explore the associations between RASi at discharge and mortality.</p><p><strong>Results: </strong>During the median follow-up time of 2.26 (1.70; 3.24) years, higher mortality rate was observed in the CI-AKI group compared to the non-CI-AKI group (18.3% vs 8.9%, <i>p</i> = 0.002). Among HF patients with CI-AKI, after adjusting for confounding factors, the association was not significant between RASi prescription at discharge and mortality (HR: 0.39, 95%CI: 0.12-1.31, <i>p</i> = 0.128), while it was among those without CI-AKI (HR: 0.39, 95%CI: 0.18-0.84, <i>p</i> = 0.016).</p><p><strong>Conclusion: </strong>RASi prescription at discharge for HF patients complicating CI-AKI tended to be ineffective, while it benefited those without CI-AKI. Further randomized evidence is needed to confirm this trend.</p>","PeriodicalId":17330,"journal":{"name":"Journal of the Renin-Angiotensin-Aldosterone System","volume":"21 4","pages":"1470320320979795"},"PeriodicalIF":4.1000,"publicationDate":"2020-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1470320320979795","citationCount":"1","resultStr":"{\"title\":\"Impact of contrast-induced acute kidney injury on the association between renin-angiotensin system inhibitors and long-term mortality in heart failure patients.\",\"authors\":\"Li Lei, Yulu Huang, Zhaodong Guo, Feier Song, Yibo He, Jin Liu, Guoli Sun, Bowen Liu, Pengyuan Chen, Jianbin Zhao, Dengxuan Wu, Yan Xue, Wenhe Yan, Zefeng Lin, Xiuqiong Huang, Guanzhong Chen, Shiqun Chen, Yong Liu, Jiyan Chen\",\"doi\":\"10.1177/1470320320979795\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Renin-angiotensin system inhibitors (RASi) reduce mortality among heart failure (HF) patients, but their effect among those complicating contrast-induced acute kidney injury (CI-AKI) remains unexplored. We aimed to investigate whether the relationship between RASi prescription at discharge and mortality differs between HF patients with or without CI-AKI following coronary angiography (CAG).</p><p><strong>Methods: </strong>About 596 HF patients from an observational cohort were divided into a CI-AKI group (<i>n</i> = 104) and a non-CI-AKI group (<i>n</i> = 492) based on whether they had CI-AKI following CAG. The endpoint was all-cause mortality. Multivariable Cox regression was performed in each group to explore the associations between RASi at discharge and mortality.</p><p><strong>Results: </strong>During the median follow-up time of 2.26 (1.70; 3.24) years, higher mortality rate was observed in the CI-AKI group compared to the non-CI-AKI group (18.3% vs 8.9%, <i>p</i> = 0.002). Among HF patients with CI-AKI, after adjusting for confounding factors, the association was not significant between RASi prescription at discharge and mortality (HR: 0.39, 95%CI: 0.12-1.31, <i>p</i> = 0.128), while it was among those without CI-AKI (HR: 0.39, 95%CI: 0.18-0.84, <i>p</i> = 0.016).</p><p><strong>Conclusion: </strong>RASi prescription at discharge for HF patients complicating CI-AKI tended to be ineffective, while it benefited those without CI-AKI. Further randomized evidence is needed to confirm this trend.</p>\",\"PeriodicalId\":17330,\"journal\":{\"name\":\"Journal of the Renin-Angiotensin-Aldosterone System\",\"volume\":\"21 4\",\"pages\":\"1470320320979795\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2020-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1470320320979795\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Renin-Angiotensin-Aldosterone System\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/1470320320979795\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Renin-Angiotensin-Aldosterone System","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/1470320320979795","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 1
摘要
导论:肾素-血管紧张素系统抑制剂(RASi)可降低心力衰竭(HF)患者的死亡率,但其在合并造反差剂诱导的急性肾损伤(CI-AKI)患者中的作用仍未研究。我们的目的是研究在有或没有冠状动脉造影(CAG)的HF患者中,出院时RASi处方与死亡率之间的关系是否不同。方法:根据CAG后是否有CI-AKI,将596例HF患者分为CI-AKI组(n = 104)和非CI-AKI组(n = 492)。终点是全因死亡率。对每组进行多变量Cox回归,探讨出院时RASi与死亡率之间的关系。结果:中位随访时间为2.26 (1.70;3.24)年,CI-AKI组的死亡率高于非CI-AKI组(18.3% vs 8.9%, p = 0.002)。在合并CI-AKI的HF患者中,校正混杂因素后,出院时RASi处方与死亡率的相关性不显著(HR: 0.39, 95%CI: 0.12-1.31, p = 0.128),而在未合并CI-AKI的HF患者中相关性显著(HR: 0.39, 95%CI: 0.18-0.84, p = 0.016)。结论:对于合并CI-AKI的HF患者,出院时开具RASi处方往往无效,而对未合并CI-AKI的患者则有利。需要进一步的随机证据来证实这一趋势。
Impact of contrast-induced acute kidney injury on the association between renin-angiotensin system inhibitors and long-term mortality in heart failure patients.
Introduction: Renin-angiotensin system inhibitors (RASi) reduce mortality among heart failure (HF) patients, but their effect among those complicating contrast-induced acute kidney injury (CI-AKI) remains unexplored. We aimed to investigate whether the relationship between RASi prescription at discharge and mortality differs between HF patients with or without CI-AKI following coronary angiography (CAG).
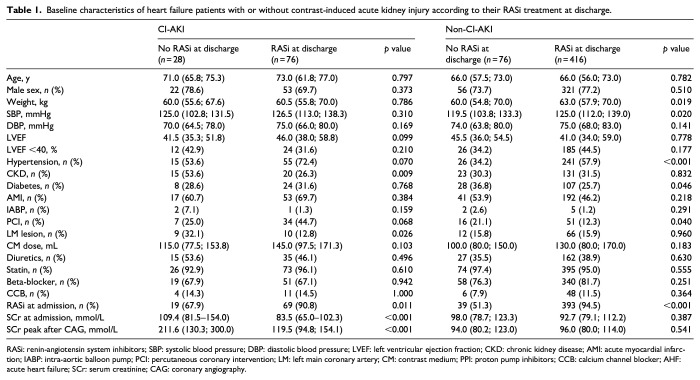
Methods: About 596 HF patients from an observational cohort were divided into a CI-AKI group (n = 104) and a non-CI-AKI group (n = 492) based on whether they had CI-AKI following CAG. The endpoint was all-cause mortality. Multivariable Cox regression was performed in each group to explore the associations between RASi at discharge and mortality.
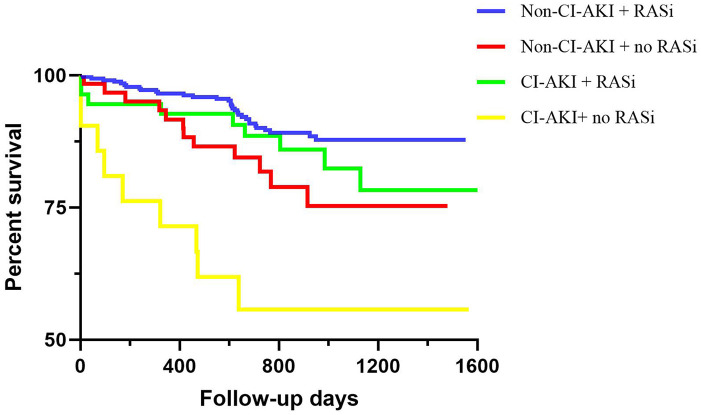
Results: During the median follow-up time of 2.26 (1.70; 3.24) years, higher mortality rate was observed in the CI-AKI group compared to the non-CI-AKI group (18.3% vs 8.9%, p = 0.002). Among HF patients with CI-AKI, after adjusting for confounding factors, the association was not significant between RASi prescription at discharge and mortality (HR: 0.39, 95%CI: 0.12-1.31, p = 0.128), while it was among those without CI-AKI (HR: 0.39, 95%CI: 0.18-0.84, p = 0.016).
Conclusion: RASi prescription at discharge for HF patients complicating CI-AKI tended to be ineffective, while it benefited those without CI-AKI. Further randomized evidence is needed to confirm this trend.
期刊介绍:
JRAAS is a peer-reviewed, open access journal, serving as a resource for biomedical professionals, primarily with an active interest in the renin-angiotensin-aldosterone system in humans and other mammals. It publishes original research and reviews on the normal and abnormal function of this system and its pharmacology and therapeutics, mostly in a cardiovascular context but including research in all areas where this system is present, including the brain, lungs and gastro-intestinal tract.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
