{"title":"放射治疗初治患者纳尔逊综合征对帕西肽的快速反应。","authors":"Xin He, Joanna L Spencer-Segal","doi":"10.1186/s40842-020-00110-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nelson's syndrome is a well-described complication following bilateral adrenalectomy for management of Cushing's disease. There is no consensus on optimal management of Nelson's syndrome, characterized by the triad of pituitary corticotroph adenoma growth, elevated serum adrenocorticotropic hormone, and skin hyperpigmentation. Medical therapy with a variety of drug classes have been studied. One potentially promising drug already approved for Cushing's disease is pasireotide, a somatostatin analog with affinity for multiple somatostatin receptors, including subtype 5, the most highly expressed receptor on corticotroph tumors.</p><p><strong>Case presentation: </strong>A 24-year-old female was diagnosed with Cushing's disease with initial ACTH levels around 700-800 pg/mL. She underwent transsphenoidal surgery without remission, followed by bilateral adrenalectomy. Over the subsequent 3 years, the patient developed skin hyperpigmentation, recurrent elevations of ACTH, and tumor recurrence requiring two additional transsphenoidal surgeries. After her third transsphenoidal resection, ACTH normalized, no residual tumor was seen on radiology, and the patient's skin hyperpigmentation improved. She then had an uncomplicated full-term pregnancy, during which ACTH levels remained within normal limits. One month after delivery, ACTH levels began rising to a peak at 5,935 pg/mL. Imaging revealed two new bilateral pituitary adenomas, measuring 14 mm on the left, and 7 mm on the right. She was then started on pasireotide. After two months of therapy, ACTH decreased to 609 pg/mL, and repeat pituitary MRI showed interval decrease in size of both pituitary adenomas to 13 mm on the left and 6 mm on the right.</p><p><strong>Conclusion: </strong>We report the protracted course of a young female with several recurrences of Nelson's syndrome following bilateral adrenalectomy and multiple transsphenoidal surgeries, who ultimately responded to pasireotide. Unique features of her case not described previously are the response to pasireotide in a radiotherapy-naive patient, as well as the rapid radiologic response to therapy. Her history illustrates the unresolved challenges of Nelson's syndrome and the continued need for additional studies to identify optimal management.</p>","PeriodicalId":56339,"journal":{"name":"Clinical Diabetes and Endocrinology","volume":"6 1","pages":"22"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40842-020-00110-7","citationCount":"5","resultStr":"{\"title\":\"Rapid response of Nelson's syndrome to pasireotide in radiotherapy-naive patient.\",\"authors\":\"Xin He, Joanna L Spencer-Segal\",\"doi\":\"10.1186/s40842-020-00110-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Nelson's syndrome is a well-described complication following bilateral adrenalectomy for management of Cushing's disease. There is no consensus on optimal management of Nelson's syndrome, characterized by the triad of pituitary corticotroph adenoma growth, elevated serum adrenocorticotropic hormone, and skin hyperpigmentation. Medical therapy with a variety of drug classes have been studied. One potentially promising drug already approved for Cushing's disease is pasireotide, a somatostatin analog with affinity for multiple somatostatin receptors, including subtype 5, the most highly expressed receptor on corticotroph tumors.</p><p><strong>Case presentation: </strong>A 24-year-old female was diagnosed with Cushing's disease with initial ACTH levels around 700-800 pg/mL. She underwent transsphenoidal surgery without remission, followed by bilateral adrenalectomy. Over the subsequent 3 years, the patient developed skin hyperpigmentation, recurrent elevations of ACTH, and tumor recurrence requiring two additional transsphenoidal surgeries. After her third transsphenoidal resection, ACTH normalized, no residual tumor was seen on radiology, and the patient's skin hyperpigmentation improved. She then had an uncomplicated full-term pregnancy, during which ACTH levels remained within normal limits. One month after delivery, ACTH levels began rising to a peak at 5,935 pg/mL. Imaging revealed two new bilateral pituitary adenomas, measuring 14 mm on the left, and 7 mm on the right. She was then started on pasireotide. After two months of therapy, ACTH decreased to 609 pg/mL, and repeat pituitary MRI showed interval decrease in size of both pituitary adenomas to 13 mm on the left and 6 mm on the right.</p><p><strong>Conclusion: </strong>We report the protracted course of a young female with several recurrences of Nelson's syndrome following bilateral adrenalectomy and multiple transsphenoidal surgeries, who ultimately responded to pasireotide. Unique features of her case not described previously are the response to pasireotide in a radiotherapy-naive patient, as well as the rapid radiologic response to therapy. Her history illustrates the unresolved challenges of Nelson's syndrome and the continued need for additional studies to identify optimal management.</p>\",\"PeriodicalId\":56339,\"journal\":{\"name\":\"Clinical Diabetes and Endocrinology\",\"volume\":\"6 1\",\"pages\":\"22\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s40842-020-00110-7\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Diabetes and Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40842-020-00110-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Diabetes and Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40842-020-00110-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Rapid response of Nelson's syndrome to pasireotide in radiotherapy-naive patient.
Background: Nelson's syndrome is a well-described complication following bilateral adrenalectomy for management of Cushing's disease. There is no consensus on optimal management of Nelson's syndrome, characterized by the triad of pituitary corticotroph adenoma growth, elevated serum adrenocorticotropic hormone, and skin hyperpigmentation. Medical therapy with a variety of drug classes have been studied. One potentially promising drug already approved for Cushing's disease is pasireotide, a somatostatin analog with affinity for multiple somatostatin receptors, including subtype 5, the most highly expressed receptor on corticotroph tumors.
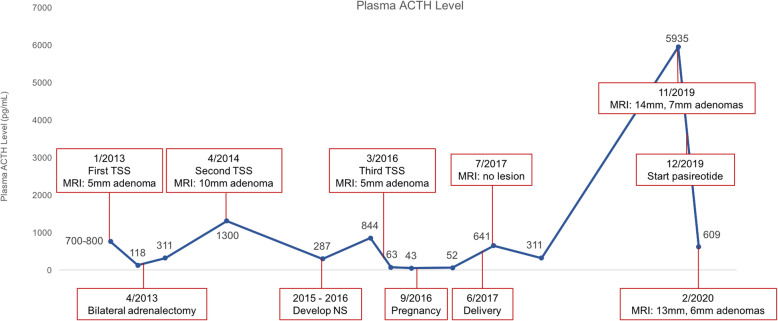
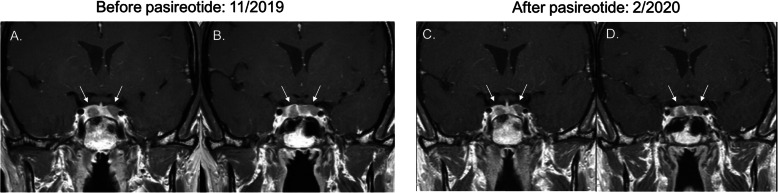
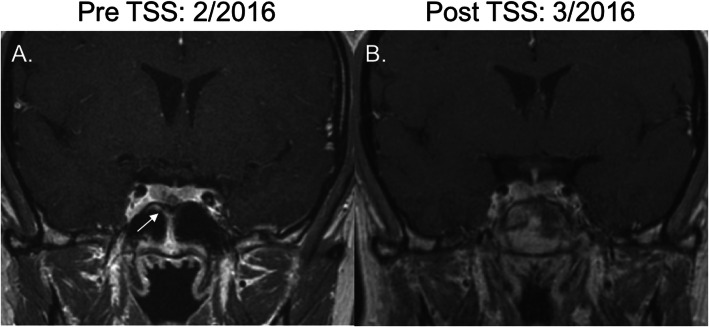
Case presentation: A 24-year-old female was diagnosed with Cushing's disease with initial ACTH levels around 700-800 pg/mL. She underwent transsphenoidal surgery without remission, followed by bilateral adrenalectomy. Over the subsequent 3 years, the patient developed skin hyperpigmentation, recurrent elevations of ACTH, and tumor recurrence requiring two additional transsphenoidal surgeries. After her third transsphenoidal resection, ACTH normalized, no residual tumor was seen on radiology, and the patient's skin hyperpigmentation improved. She then had an uncomplicated full-term pregnancy, during which ACTH levels remained within normal limits. One month after delivery, ACTH levels began rising to a peak at 5,935 pg/mL. Imaging revealed two new bilateral pituitary adenomas, measuring 14 mm on the left, and 7 mm on the right. She was then started on pasireotide. After two months of therapy, ACTH decreased to 609 pg/mL, and repeat pituitary MRI showed interval decrease in size of both pituitary adenomas to 13 mm on the left and 6 mm on the right.
Conclusion: We report the protracted course of a young female with several recurrences of Nelson's syndrome following bilateral adrenalectomy and multiple transsphenoidal surgeries, who ultimately responded to pasireotide. Unique features of her case not described previously are the response to pasireotide in a radiotherapy-naive patient, as well as the rapid radiologic response to therapy. Her history illustrates the unresolved challenges of Nelson's syndrome and the continued need for additional studies to identify optimal management.
期刊介绍:
Clinical Diabetes and Endocrinology is an open access journal publishing within the field of diabetes and endocrine disease. The journal aims to provide a widely available resource for people working within the field of diabetes and endocrinology, in order to improve the care of people affected by these conditions. The audience includes, but is not limited to, physicians, researchers, nurses, nutritionists, pharmacists, podiatrists, psychologists, epidemiologists, exercise physiologists and health care researchers. Research articles include patient-based research (clinical trials, clinical studies, and others), translational research (translation of basic science to clinical practice, translation of clinical practice to policy and others), as well as epidemiology and health care research. Clinical articles include case reports, case seminars, consensus statements, clinical practice guidelines and evidence-based medicine. Only articles considered to contribute new knowledge to the field will be considered for publication.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
