A Khan, E Omakobia, S Hasnie, R Barton, P Gopalan, V Oktseloglou, I Smith
{"title":"以左侧颞下颌关节为中心的真菌性坏死性外耳道炎罕见病例","authors":"A Khan, E Omakobia, S Hasnie, R Barton, P Gopalan, V Oktseloglou, I Smith","doi":"10.1155/2020/8874754","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Necrotising otitis externa (NOE) is a rare life-threatening complication of simple otitis externa which can be difficult to diagnose and manage. It is very rarely centred on the temporomandibular joint (TMJ). Fungi cause NOE in approximately 5-20% of patients, and a high index of suspicion is required for diagnosis, particularly when there is no improvement with prolonged topical and intravenous antibiotic therapy.</p><p><strong>Objective: </strong>To report a novel case of fungal NOE centred on the left TMJ in an immunocompromised adult male with a focus on investigations and optimal management. <i>Case Report</i>. A 67-year-old male with comorbid chronic renal impairment presented to our otolaryngology department with prolonged left otalgia and otorrhoea. Subsequent cross-sectional imaging demonstrated left NOE centred on the TMJ. Poor resolution with prolonged courses of systemic and topical anti-pseudomonal antibiotics prompted maxillofacial surgical input for left TMJ exploration, washout, and biopsy from the joint capsule. The causative organism was identified as <i>Aspergillus flavus</i> on PCR analysis. The patient was successfully treated with oral posaconazole and repeated topical insertions of amphotericin B-soaked ribbon gauze to the left ear. <i>Discussion</i>. A combination of various imaging modalities including CT, MRI, Tc-99, and gallium-67 are utilised in clinical practice both to diagnose NOE and subsequently monitor disease progression or resolution. Immunocompromised patients with confirmed fungal NOE may require a combination of treatments including surgical debridement and prolonged antifungal therapy for a number of months, if not lifelong, treatment. Initiating empirical antifungal therapy may be justified in some patients. However, this should be judged on a case-by-case basis and guided by discussion with the local microbiology and infectious diseases departments. However, there is no national guideline or consensus regarding treatment of these patients, especially in cases of fungal NOE.</p>","PeriodicalId":45872,"journal":{"name":"Case Reports in Otolaryngology","volume":"2020 ","pages":"8874754"},"PeriodicalIF":0.4000,"publicationDate":"2020-11-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7665930/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Rare Case of Fungal Necrotising Otitis Externa Centred on the Left Temporomandibular Joint.\",\"authors\":\"A Khan, E Omakobia, S Hasnie, R Barton, P Gopalan, V Oktseloglou, I Smith\",\"doi\":\"10.1155/2020/8874754\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Necrotising otitis externa (NOE) is a rare life-threatening complication of simple otitis externa which can be difficult to diagnose and manage. It is very rarely centred on the temporomandibular joint (TMJ). Fungi cause NOE in approximately 5-20% of patients, and a high index of suspicion is required for diagnosis, particularly when there is no improvement with prolonged topical and intravenous antibiotic therapy.</p><p><strong>Objective: </strong>To report a novel case of fungal NOE centred on the left TMJ in an immunocompromised adult male with a focus on investigations and optimal management. <i>Case Report</i>. A 67-year-old male with comorbid chronic renal impairment presented to our otolaryngology department with prolonged left otalgia and otorrhoea. Subsequent cross-sectional imaging demonstrated left NOE centred on the TMJ. Poor resolution with prolonged courses of systemic and topical anti-pseudomonal antibiotics prompted maxillofacial surgical input for left TMJ exploration, washout, and biopsy from the joint capsule. The causative organism was identified as <i>Aspergillus flavus</i> on PCR analysis. The patient was successfully treated with oral posaconazole and repeated topical insertions of amphotericin B-soaked ribbon gauze to the left ear. <i>Discussion</i>. A combination of various imaging modalities including CT, MRI, Tc-99, and gallium-67 are utilised in clinical practice both to diagnose NOE and subsequently monitor disease progression or resolution. Immunocompromised patients with confirmed fungal NOE may require a combination of treatments including surgical debridement and prolonged antifungal therapy for a number of months, if not lifelong, treatment. Initiating empirical antifungal therapy may be justified in some patients. However, this should be judged on a case-by-case basis and guided by discussion with the local microbiology and infectious diseases departments. However, there is no national guideline or consensus regarding treatment of these patients, especially in cases of fungal NOE.</p>\",\"PeriodicalId\":45872,\"journal\":{\"name\":\"Case Reports in Otolaryngology\",\"volume\":\"2020 \",\"pages\":\"8874754\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2020-11-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7665930/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Otolaryngology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/8874754\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Otolaryngology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/8874754","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
简介坏死性外耳道炎(NOE)是一种罕见的威胁生命的单纯性外耳道炎并发症,很难诊断和处理。它很少以颞下颌关节(TMJ)为中心。约有 5-20% 的患者由真菌引起 NOE,诊断时需要高度怀疑,尤其是在长期局部和静脉抗生素治疗无好转时:报告一例免疫力低下的成年男性左侧颞下颌关节真菌 NOE 的新病例,重点是检查和优化治疗。病例报告。一名 67 岁的男性患者因长期左侧耳痛和耳鸣到我院耳鼻喉科就诊。随后的横断面成像显示左侧 NOE 以颞下颌关节为中心。经过长时间的全身和局部抗假性抗生素治疗后,症状缓解不佳,颌面外科决定对左侧颞下颌关节进行探查、冲洗和关节囊活检。通过 PCR 分析,确定致病菌为黄曲霉菌。患者通过口服泊沙康唑和反复在左耳局部塞入两性霉素 B 浸泡过的带状纱布获得了成功治疗。讨论。在临床实践中,包括 CT、核磁共振成像、Tc-99 和镓-67 在内的各种成像模式相结合,可用于诊断 NOE 以及随后监测疾病的进展或缓解情况。确诊为真菌性 NOE 的免疫力低下患者可能需要综合治疗,包括手术清创和长达数月(甚至终身)的抗真菌治疗。对于某些患者,启动经验性抗真菌治疗可能是合理的。不过,应根据具体情况进行判断,并与当地微生物学和传染病部门进行讨论。然而,对于这些患者的治疗,尤其是真菌 NOE 病例的治疗,目前还没有全国性的指南或共识。
A Rare Case of Fungal Necrotising Otitis Externa Centred on the Left Temporomandibular Joint.
Introduction: Necrotising otitis externa (NOE) is a rare life-threatening complication of simple otitis externa which can be difficult to diagnose and manage. It is very rarely centred on the temporomandibular joint (TMJ). Fungi cause NOE in approximately 5-20% of patients, and a high index of suspicion is required for diagnosis, particularly when there is no improvement with prolonged topical and intravenous antibiotic therapy.
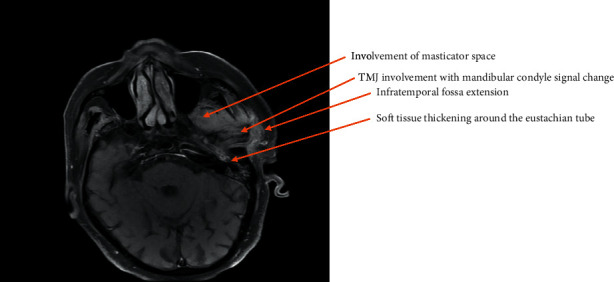
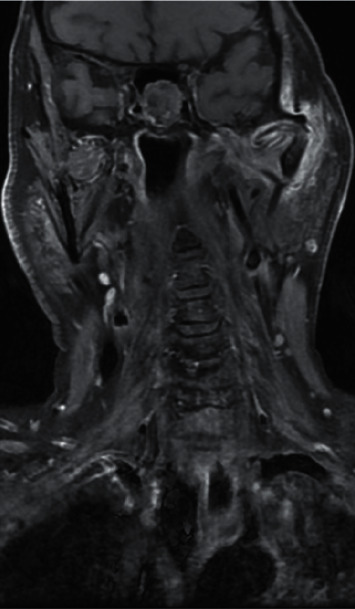
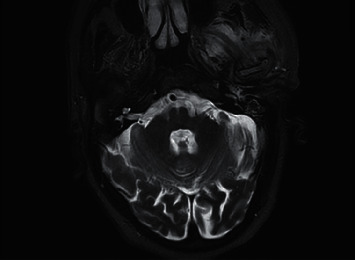
Objective: To report a novel case of fungal NOE centred on the left TMJ in an immunocompromised adult male with a focus on investigations and optimal management. Case Report. A 67-year-old male with comorbid chronic renal impairment presented to our otolaryngology department with prolonged left otalgia and otorrhoea. Subsequent cross-sectional imaging demonstrated left NOE centred on the TMJ. Poor resolution with prolonged courses of systemic and topical anti-pseudomonal antibiotics prompted maxillofacial surgical input for left TMJ exploration, washout, and biopsy from the joint capsule. The causative organism was identified as Aspergillus flavus on PCR analysis. The patient was successfully treated with oral posaconazole and repeated topical insertions of amphotericin B-soaked ribbon gauze to the left ear. Discussion. A combination of various imaging modalities including CT, MRI, Tc-99, and gallium-67 are utilised in clinical practice both to diagnose NOE and subsequently monitor disease progression or resolution. Immunocompromised patients with confirmed fungal NOE may require a combination of treatments including surgical debridement and prolonged antifungal therapy for a number of months, if not lifelong, treatment. Initiating empirical antifungal therapy may be justified in some patients. However, this should be judged on a case-by-case basis and guided by discussion with the local microbiology and infectious diseases departments. However, there is no national guideline or consensus regarding treatment of these patients, especially in cases of fungal NOE.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
