Brian Burnett, Linda Street, Kristen Quinn, Jeff M Denney
{"title":"早发性胎儿生长受限:诊断途径会影响结果和病理吗?","authors":"Brian Burnett, Linda Street, Kristen Quinn, Jeff M Denney","doi":"10.33696/gynaecology.1.002","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate demographics and outcomes of maternal-fetal pairs in early onset fetal growth restriction (FGR) requiring delivery prior to 34 weeks' gestation based on ultrasound indication leading to diagnosis.</p><p><strong>Study design: </strong>This is a descriptive study of maternal-fetal pairs with early FGR diagnosed prior to 30 weeks' gestation and delivering between 22w0d and 34w0d under the care of Wake Forest University Perinatology 01/2012-12/2016. Serial ultrasounds to assess fetal growth and umbilical artery flow Doppler velocimetry were evaluated. Pairs were dichotomized into those with maternal comorbidities leading to ultrasound diagnosis, and those with ultrasound indicated only by appreciation of uterine size less than dates on exam. Patient characteristics and outcomes were tracked. Univariate and multivariate analyses were performed as appropriate.</p><p><strong>Results: </strong>56 pregnancies were identified with FGR prior to 30 weeks and subsequent delivery prior to 34 weeks. Common comorbidities present in the group with maternal comorbidities included chronic hypertension (30.5%), hypertensive disorders of pregnancy (36.1%), preexisting diabetes (13.9%), gestational diabetes (5.6%). None of the women in the S<D group developed hypertensive disorders of pregnancy or GDM. Other background characteristics were similar. Pregnancies evaluated for size less than dates were diagnosed on average 3 weeks later in gestation, had higher incidence of reverse end diastolic flow on Doppler evaluation both at diagnosis (80% vs. 22.9%, p=0.01, OR 0.08 (<0.01,0.74) and were more likely to be delivered for an urgent indication. Both groups of babies had similar survival to discharge rates and length of stay in the NICU. A subanalysis evaluating only babies with abnormal Doppler studies showed a shorter diagnosis to delivery interval and continued to show increased risk of urgent delivery due to fetal status in those pregnancies diagnosed based on size<dates.</p><p><strong>Conclusion: </strong>Women measuring size less than dates in the mid-trimester should be evaluated by ultrasound without delays. Early FGR carries a high mortality rate in all cases and in our pilot data, women measuring small were diagnosed later with fetal growth restriction and may represent a severe phenotype with poor fetal-placental circulation. These pregnancies often met criteria for urgent delivery in a short time frame, especially if abnormal umbilical artery Doppler velocimetry was noted.</p>","PeriodicalId":93076,"journal":{"name":"Archives of obstetrics and gynaecology","volume":"1 1","pages":"5-12"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7671592/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early Onset Fetal Growth Restriction: Does Path to Diagnosis Impact Outcomes and Pathology?\",\"authors\":\"Brian Burnett, Linda Street, Kristen Quinn, Jeff M Denney\",\"doi\":\"10.33696/gynaecology.1.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To evaluate demographics and outcomes of maternal-fetal pairs in early onset fetal growth restriction (FGR) requiring delivery prior to 34 weeks' gestation based on ultrasound indication leading to diagnosis.</p><p><strong>Study design: </strong>This is a descriptive study of maternal-fetal pairs with early FGR diagnosed prior to 30 weeks' gestation and delivering between 22w0d and 34w0d under the care of Wake Forest University Perinatology 01/2012-12/2016. Serial ultrasounds to assess fetal growth and umbilical artery flow Doppler velocimetry were evaluated. Pairs were dichotomized into those with maternal comorbidities leading to ultrasound diagnosis, and those with ultrasound indicated only by appreciation of uterine size less than dates on exam. Patient characteristics and outcomes were tracked. Univariate and multivariate analyses were performed as appropriate.</p><p><strong>Results: </strong>56 pregnancies were identified with FGR prior to 30 weeks and subsequent delivery prior to 34 weeks. Common comorbidities present in the group with maternal comorbidities included chronic hypertension (30.5%), hypertensive disorders of pregnancy (36.1%), preexisting diabetes (13.9%), gestational diabetes (5.6%). None of the women in the S<D group developed hypertensive disorders of pregnancy or GDM. Other background characteristics were similar. Pregnancies evaluated for size less than dates were diagnosed on average 3 weeks later in gestation, had higher incidence of reverse end diastolic flow on Doppler evaluation both at diagnosis (80% vs. 22.9%, p=0.01, OR 0.08 (<0.01,0.74) and were more likely to be delivered for an urgent indication. Both groups of babies had similar survival to discharge rates and length of stay in the NICU. A subanalysis evaluating only babies with abnormal Doppler studies showed a shorter diagnosis to delivery interval and continued to show increased risk of urgent delivery due to fetal status in those pregnancies diagnosed based on size<dates.</p><p><strong>Conclusion: </strong>Women measuring size less than dates in the mid-trimester should be evaluated by ultrasound without delays. Early FGR carries a high mortality rate in all cases and in our pilot data, women measuring small were diagnosed later with fetal growth restriction and may represent a severe phenotype with poor fetal-placental circulation. These pregnancies often met criteria for urgent delivery in a short time frame, especially if abnormal umbilical artery Doppler velocimetry was noted.</p>\",\"PeriodicalId\":93076,\"journal\":{\"name\":\"Archives of obstetrics and gynaecology\",\"volume\":\"1 1\",\"pages\":\"5-12\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7671592/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of obstetrics and gynaecology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.33696/gynaecology.1.002\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of obstetrics and gynaecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.33696/gynaecology.1.002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Early Onset Fetal Growth Restriction: Does Path to Diagnosis Impact Outcomes and Pathology?
Objective: To evaluate demographics and outcomes of maternal-fetal pairs in early onset fetal growth restriction (FGR) requiring delivery prior to 34 weeks' gestation based on ultrasound indication leading to diagnosis.
Study design: This is a descriptive study of maternal-fetal pairs with early FGR diagnosed prior to 30 weeks' gestation and delivering between 22w0d and 34w0d under the care of Wake Forest University Perinatology 01/2012-12/2016. Serial ultrasounds to assess fetal growth and umbilical artery flow Doppler velocimetry were evaluated. Pairs were dichotomized into those with maternal comorbidities leading to ultrasound diagnosis, and those with ultrasound indicated only by appreciation of uterine size less than dates on exam. Patient characteristics and outcomes were tracked. Univariate and multivariate analyses were performed as appropriate.
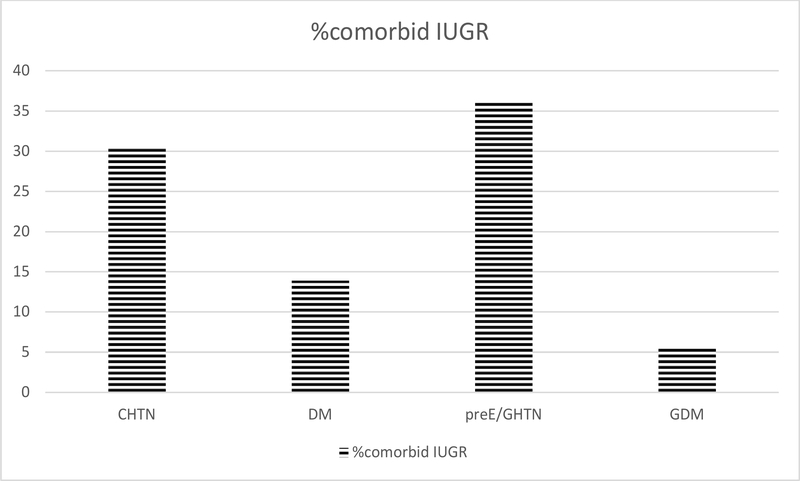
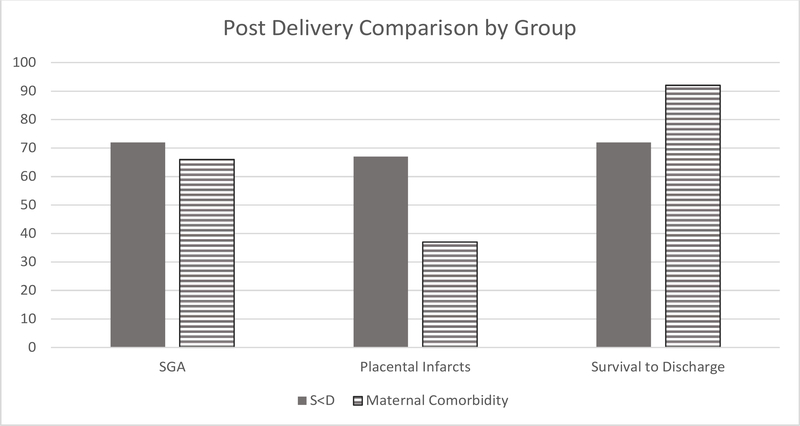
Results: 56 pregnancies were identified with FGR prior to 30 weeks and subsequent delivery prior to 34 weeks. Common comorbidities present in the group with maternal comorbidities included chronic hypertension (30.5%), hypertensive disorders of pregnancy (36.1%), preexisting diabetes (13.9%), gestational diabetes (5.6%). None of the women in the S
Conclusion: Women measuring size less than dates in the mid-trimester should be evaluated by ultrasound without delays. Early FGR carries a high mortality rate in all cases and in our pilot data, women measuring small were diagnosed later with fetal growth restriction and may represent a severe phenotype with poor fetal-placental circulation. These pregnancies often met criteria for urgent delivery in a short time frame, especially if abnormal umbilical artery Doppler velocimetry was noted.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
