Stephanie Romutis, Bassem Matta, Jonathan Ibinson, John Hileman, Smiljana Istvanic, Asif Khalid
{"title":"结扎和自动截肢辅助EMR治疗结肠大外侧扩散肿瘤和常规息肉切除术无法治疗的息肉的安全性和有效性。","authors":"Stephanie Romutis, Bassem Matta, Jonathan Ibinson, John Hileman, Smiljana Istvanic, Asif Khalid","doi":"10.1177/26317745211001750","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The safety and efficacy of colonic band ligation and auto-amputation (1) as adjunct to endoscopic mucosal resection of large laterally spreading tumors and (2) for polyps not amenable to routine polypectomy due to polyp burden or difficult location remain unknown.</p><p><strong>Methods: </strong>An institutional review board-approved retrospective single-institution study was undertaken of patients undergoing colonic band ligation and auto-amputation from 2014 to date. Patients with indications of 'endoscopic mucosal resection for laterally spreading tumors' and 'polyp not amenable to snare polypectomy' were included in the study. Data were collected on patient demographics, colonoscopy details (laterally spreading tumors/polyp characteristics, therapies applied, complications), pathology results, and follow-up (polyp eradication based on endoscopic appearance and biopsy results).</p><p><strong>Results: </strong><i>Patients undergoing endoscopic mucosal resection for laterally spreading tumors</i>: Thirty-two patients (31 males, aged 68 ± 9.17 years) underwent endoscopic mucosal resection-band ligation and auto-amputation of 34 laterally spreading tumors (40 ± 10.9 mm). A median of 2 ± 1.09 bands were placed. Follow-up colonoscopy and biopsy results confirmed complete eradication in 21 laterally spreading tumors (70%). Nine (30%) laterally spreading tumors required additional endoscopic therapy to achieve complete eradication. Four (13%) patients underwent surgery for cancer, and two of them had resection specimens negative for cancer or residual adenoma. One patient suffered post-polypectomy syndrome. <i>Patients undergoing band ligation and auto-amputation for polyps not amenable to snare polypectomy</i>: Seven patients underwent band ligation and auto-amputation due to serrated polyposis syndrome (one patient) and innumerable polyps, or polyps in difficult locations (extension into diverticula: two patients; terminal ileum: two patients; appendiceal orifice: one patient; anal canal: one patient). The patient with serrated polyposis syndrome achieved dramatic decrease in polyp burden, but not eradication. Follow-up in five of the six remaining patients documented polyp eradication. The patient with serrated polyposis syndrome suffered from rectal pain and tenesmus following placement of 18 bands.</p><p><strong>Conclusions: </strong>Band ligation and auto-amputation in the colon may be a safe and effective adjunct to current endoscopic mucosal resection and polypectomy methods and warrants further study.</p><p><strong>Plain language summary: </strong>Colonoscopy with rubber band placement to aid in complete removal of large polyps and polyps in technically challenging locationsColonoscopy is a commonly performed procedure for the early detection of colon and rectal cancer, and prevention through polyp removal.During colonoscopy, sometimes situations are encountered making polyp removal difficult. These can include the presence of larger polyps or the location of a polyp in an area that makes removal technically challenging or high risk.A particularly challenging situation arises when after extensive effort there is still polyp tissue remaining that cannot be removed using routine techniques. We are interested in exploring a technique which involves the placement of a rubber band after sucking a small area of the colon lining into a cap loaded onto the tip of the colonoscope. With time the rubber band strangulates the tissue and falls off along with captured tissue and passes out of the colon naturally.To assess the effectives of this technique we studied patients that have undergone this procedure at our GI unit. We identified 32 patients with 34 large polyps between 4cm to 6cm that we placed rubber bands on polyp tissue after we were unable to completely remove the polyp. On their follow up colonoscopy, complete polyp removal was successful in 21 polyps. We were also able to achieve complete polyp removal in 9 of the remaining large polyps after additional treatment. Four patients underwent surgery because cancer was found in analysis of polyp tissue.In 5 of 6 patients with polyps in difficult locations (e.g. partly within the lumen of the appendix), placement of a rubber band led to complete removal of polyp tissue.Two patients in our study population had mild adverse events that were managed with simple measures.We believe our results show promise for our described technique and this technique should be tested in larger studies.</p>","PeriodicalId":40947,"journal":{"name":"Therapeutic Advances in Gastrointestinal Endoscopy","volume":"14 ","pages":"26317745211001750"},"PeriodicalIF":3.0000,"publicationDate":"2021-03-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/26317745211001750","citationCount":"0","resultStr":"{\"title\":\"Safety and efficacy of band ligation and auto-amputation as adjunct to EMR of colonic large laterally spreading tumors, and polyps not amenable to routine polypectomy.\",\"authors\":\"Stephanie Romutis, Bassem Matta, Jonathan Ibinson, John Hileman, Smiljana Istvanic, Asif Khalid\",\"doi\":\"10.1177/26317745211001750\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The safety and efficacy of colonic band ligation and auto-amputation (1) as adjunct to endoscopic mucosal resection of large laterally spreading tumors and (2) for polyps not amenable to routine polypectomy due to polyp burden or difficult location remain unknown.</p><p><strong>Methods: </strong>An institutional review board-approved retrospective single-institution study was undertaken of patients undergoing colonic band ligation and auto-amputation from 2014 to date. Patients with indications of 'endoscopic mucosal resection for laterally spreading tumors' and 'polyp not amenable to snare polypectomy' were included in the study. Data were collected on patient demographics, colonoscopy details (laterally spreading tumors/polyp characteristics, therapies applied, complications), pathology results, and follow-up (polyp eradication based on endoscopic appearance and biopsy results).</p><p><strong>Results: </strong><i>Patients undergoing endoscopic mucosal resection for laterally spreading tumors</i>: Thirty-two patients (31 males, aged 68 ± 9.17 years) underwent endoscopic mucosal resection-band ligation and auto-amputation of 34 laterally spreading tumors (40 ± 10.9 mm). A median of 2 ± 1.09 bands were placed. Follow-up colonoscopy and biopsy results confirmed complete eradication in 21 laterally spreading tumors (70%). Nine (30%) laterally spreading tumors required additional endoscopic therapy to achieve complete eradication. Four (13%) patients underwent surgery for cancer, and two of them had resection specimens negative for cancer or residual adenoma. One patient suffered post-polypectomy syndrome. <i>Patients undergoing band ligation and auto-amputation for polyps not amenable to snare polypectomy</i>: Seven patients underwent band ligation and auto-amputation due to serrated polyposis syndrome (one patient) and innumerable polyps, or polyps in difficult locations (extension into diverticula: two patients; terminal ileum: two patients; appendiceal orifice: one patient; anal canal: one patient). The patient with serrated polyposis syndrome achieved dramatic decrease in polyp burden, but not eradication. Follow-up in five of the six remaining patients documented polyp eradication. The patient with serrated polyposis syndrome suffered from rectal pain and tenesmus following placement of 18 bands.</p><p><strong>Conclusions: </strong>Band ligation and auto-amputation in the colon may be a safe and effective adjunct to current endoscopic mucosal resection and polypectomy methods and warrants further study.</p><p><strong>Plain language summary: </strong>Colonoscopy with rubber band placement to aid in complete removal of large polyps and polyps in technically challenging locationsColonoscopy is a commonly performed procedure for the early detection of colon and rectal cancer, and prevention through polyp removal.During colonoscopy, sometimes situations are encountered making polyp removal difficult. These can include the presence of larger polyps or the location of a polyp in an area that makes removal technically challenging or high risk.A particularly challenging situation arises when after extensive effort there is still polyp tissue remaining that cannot be removed using routine techniques. We are interested in exploring a technique which involves the placement of a rubber band after sucking a small area of the colon lining into a cap loaded onto the tip of the colonoscope. With time the rubber band strangulates the tissue and falls off along with captured tissue and passes out of the colon naturally.To assess the effectives of this technique we studied patients that have undergone this procedure at our GI unit. We identified 32 patients with 34 large polyps between 4cm to 6cm that we placed rubber bands on polyp tissue after we were unable to completely remove the polyp. On their follow up colonoscopy, complete polyp removal was successful in 21 polyps. We were also able to achieve complete polyp removal in 9 of the remaining large polyps after additional treatment. Four patients underwent surgery because cancer was found in analysis of polyp tissue.In 5 of 6 patients with polyps in difficult locations (e.g. partly within the lumen of the appendix), placement of a rubber band led to complete removal of polyp tissue.Two patients in our study population had mild adverse events that were managed with simple measures.We believe our results show promise for our described technique and this technique should be tested in larger studies.</p>\",\"PeriodicalId\":40947,\"journal\":{\"name\":\"Therapeutic Advances in Gastrointestinal Endoscopy\",\"volume\":\"14 \",\"pages\":\"26317745211001750\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2021-03-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/26317745211001750\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastrointestinal Endoscopy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26317745211001750\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastrointestinal Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26317745211001750","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Safety and efficacy of band ligation and auto-amputation as adjunct to EMR of colonic large laterally spreading tumors, and polyps not amenable to routine polypectomy.
Introduction: The safety and efficacy of colonic band ligation and auto-amputation (1) as adjunct to endoscopic mucosal resection of large laterally spreading tumors and (2) for polyps not amenable to routine polypectomy due to polyp burden or difficult location remain unknown.
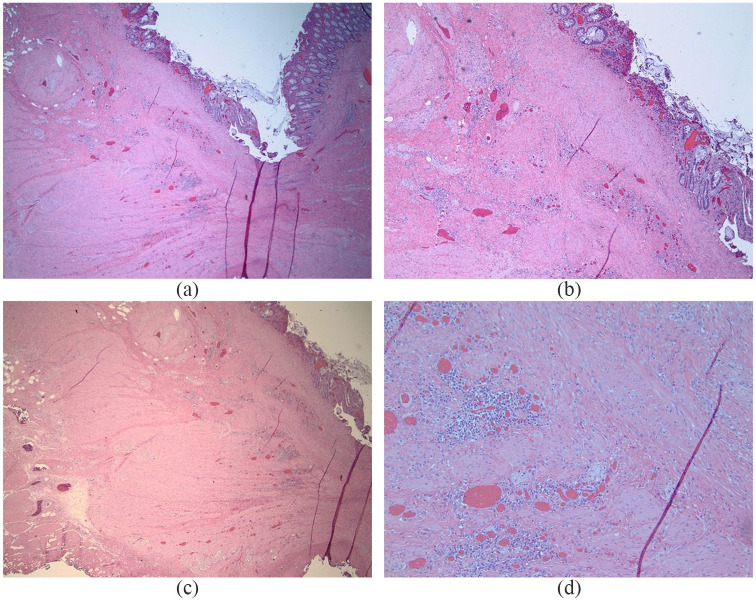
Methods: An institutional review board-approved retrospective single-institution study was undertaken of patients undergoing colonic band ligation and auto-amputation from 2014 to date. Patients with indications of 'endoscopic mucosal resection for laterally spreading tumors' and 'polyp not amenable to snare polypectomy' were included in the study. Data were collected on patient demographics, colonoscopy details (laterally spreading tumors/polyp characteristics, therapies applied, complications), pathology results, and follow-up (polyp eradication based on endoscopic appearance and biopsy results).
Results: Patients undergoing endoscopic mucosal resection for laterally spreading tumors: Thirty-two patients (31 males, aged 68 ± 9.17 years) underwent endoscopic mucosal resection-band ligation and auto-amputation of 34 laterally spreading tumors (40 ± 10.9 mm). A median of 2 ± 1.09 bands were placed. Follow-up colonoscopy and biopsy results confirmed complete eradication in 21 laterally spreading tumors (70%). Nine (30%) laterally spreading tumors required additional endoscopic therapy to achieve complete eradication. Four (13%) patients underwent surgery for cancer, and two of them had resection specimens negative for cancer or residual adenoma. One patient suffered post-polypectomy syndrome. Patients undergoing band ligation and auto-amputation for polyps not amenable to snare polypectomy: Seven patients underwent band ligation and auto-amputation due to serrated polyposis syndrome (one patient) and innumerable polyps, or polyps in difficult locations (extension into diverticula: two patients; terminal ileum: two patients; appendiceal orifice: one patient; anal canal: one patient). The patient with serrated polyposis syndrome achieved dramatic decrease in polyp burden, but not eradication. Follow-up in five of the six remaining patients documented polyp eradication. The patient with serrated polyposis syndrome suffered from rectal pain and tenesmus following placement of 18 bands.
Conclusions: Band ligation and auto-amputation in the colon may be a safe and effective adjunct to current endoscopic mucosal resection and polypectomy methods and warrants further study.
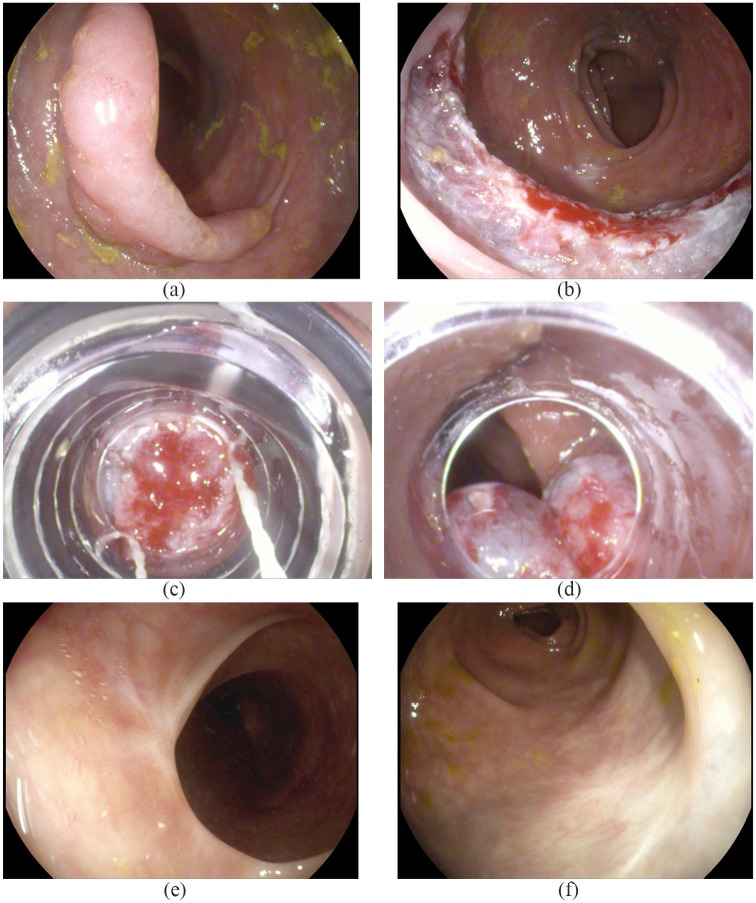
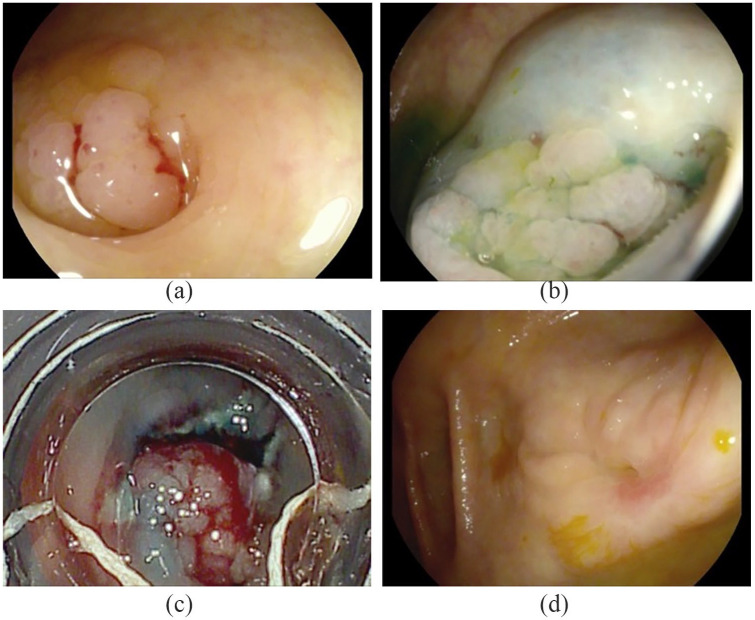
Plain language summary: Colonoscopy with rubber band placement to aid in complete removal of large polyps and polyps in technically challenging locationsColonoscopy is a commonly performed procedure for the early detection of colon and rectal cancer, and prevention through polyp removal.During colonoscopy, sometimes situations are encountered making polyp removal difficult. These can include the presence of larger polyps or the location of a polyp in an area that makes removal technically challenging or high risk.A particularly challenging situation arises when after extensive effort there is still polyp tissue remaining that cannot be removed using routine techniques. We are interested in exploring a technique which involves the placement of a rubber band after sucking a small area of the colon lining into a cap loaded onto the tip of the colonoscope. With time the rubber band strangulates the tissue and falls off along with captured tissue and passes out of the colon naturally.To assess the effectives of this technique we studied patients that have undergone this procedure at our GI unit. We identified 32 patients with 34 large polyps between 4cm to 6cm that we placed rubber bands on polyp tissue after we were unable to completely remove the polyp. On their follow up colonoscopy, complete polyp removal was successful in 21 polyps. We were also able to achieve complete polyp removal in 9 of the remaining large polyps after additional treatment. Four patients underwent surgery because cancer was found in analysis of polyp tissue.In 5 of 6 patients with polyps in difficult locations (e.g. partly within the lumen of the appendix), placement of a rubber band led to complete removal of polyp tissue.Two patients in our study population had mild adverse events that were managed with simple measures.We believe our results show promise for our described technique and this technique should be tested in larger studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
