{"title":"疾病预防控制中心 2016 年阿片类药物指南发布前后的阿片类药物和非阿片类药物镇痛处方。","authors":"William Encinosa, Didem Bernard, Thomas M Selden","doi":"10.1007/s10754-021-09307-4","DOIUrl":null,"url":null,"abstract":"<p><p>The U.S. has addressed the opioid crisis using a two-front approach: state regulations limiting opioid prescriptions for acute pain patients, and voluntary federal CDC guidelines on shifting chronic pain patients to lower opioid doses and non-opioids. No opioid policy research to date has accounted for this two-pronged approach in their research design. We develop a theory of physician prescribing behavior under this two-pronged incentive structure. Using the Medical Expenditure Panel Survey, we empirically corroborate the theory: regulations and guidelines have the intended effects of reducing opioid prescriptions for acute and chronic pain, respectively, as well as the predicted unintended effects-income effects cause regulations on acute pain treatment to increase chronic pain opioid prescriptions and the chronic pain treatment guidelines spillover to reduce opioids for acute pain. Moreover, we find that the guidelines worked as intended in terms of the reduced usage, with chronic pain patients shifting to non-opioids and also tapering opioid doses. For those who discontinued opioids under regulations and guidelines, we find no harm in terms of increased work limitations due to pain a year after discontinuing opioids. Finally, we observe an unexplained dichotomy-regulations reduce opioid use by causing fewer new starts, whereas guidelines reduce opioid use by discontinuing current users, with no impact on new starts.</p>","PeriodicalId":44403,"journal":{"name":"International Journal of Health Economics and Management","volume":"22 1","pages":"1-52"},"PeriodicalIF":1.7000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8105705/pdf/","citationCount":"0","resultStr":"{\"title\":\"Opioid and non-opioid analgesic prescribing before and after the CDC's 2016 opioid guideline.\",\"authors\":\"William Encinosa, Didem Bernard, Thomas M Selden\",\"doi\":\"10.1007/s10754-021-09307-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The U.S. has addressed the opioid crisis using a two-front approach: state regulations limiting opioid prescriptions for acute pain patients, and voluntary federal CDC guidelines on shifting chronic pain patients to lower opioid doses and non-opioids. No opioid policy research to date has accounted for this two-pronged approach in their research design. We develop a theory of physician prescribing behavior under this two-pronged incentive structure. Using the Medical Expenditure Panel Survey, we empirically corroborate the theory: regulations and guidelines have the intended effects of reducing opioid prescriptions for acute and chronic pain, respectively, as well as the predicted unintended effects-income effects cause regulations on acute pain treatment to increase chronic pain opioid prescriptions and the chronic pain treatment guidelines spillover to reduce opioids for acute pain. Moreover, we find that the guidelines worked as intended in terms of the reduced usage, with chronic pain patients shifting to non-opioids and also tapering opioid doses. For those who discontinued opioids under regulations and guidelines, we find no harm in terms of increased work limitations due to pain a year after discontinuing opioids. Finally, we observe an unexplained dichotomy-regulations reduce opioid use by causing fewer new starts, whereas guidelines reduce opioid use by discontinuing current users, with no impact on new starts.</p>\",\"PeriodicalId\":44403,\"journal\":{\"name\":\"International Journal of Health Economics and Management\",\"volume\":\"22 1\",\"pages\":\"1-52\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8105705/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Health Economics and Management\",\"FirstCategoryId\":\"96\",\"ListUrlMain\":\"https://doi.org/10.1007/s10754-021-09307-4\",\"RegionNum\":4,\"RegionCategory\":\"经济学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/5/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"BUSINESS, FINANCE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Health Economics and Management","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1007/s10754-021-09307-4","RegionNum":4,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/5/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"BUSINESS, FINANCE","Score":null,"Total":0}
Opioid and non-opioid analgesic prescribing before and after the CDC's 2016 opioid guideline.
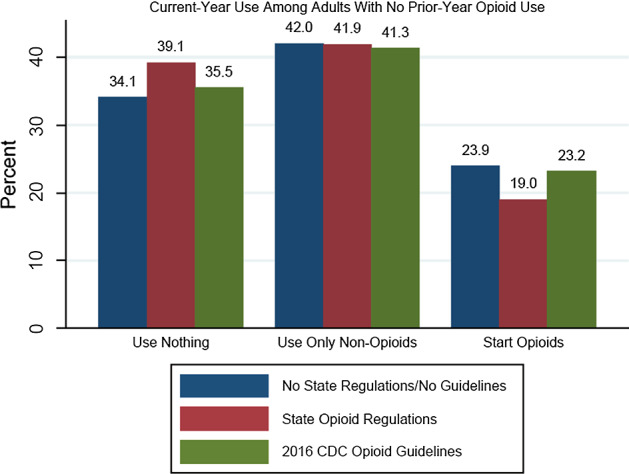
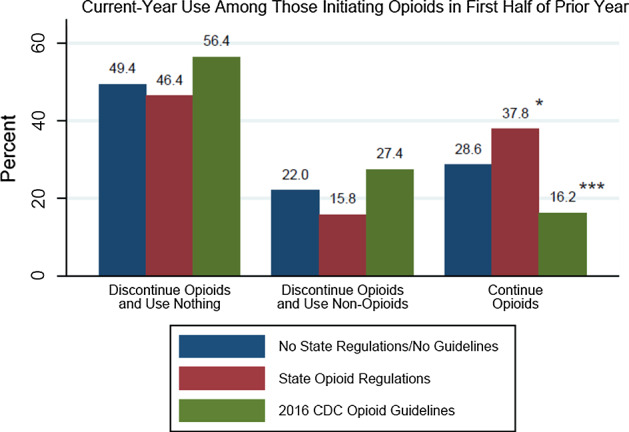
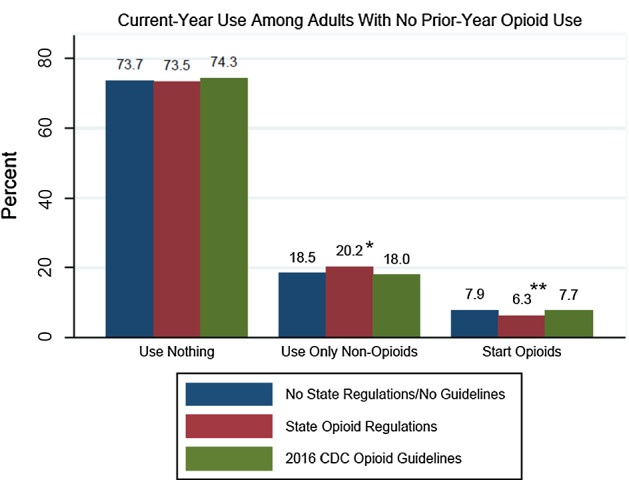
The U.S. has addressed the opioid crisis using a two-front approach: state regulations limiting opioid prescriptions for acute pain patients, and voluntary federal CDC guidelines on shifting chronic pain patients to lower opioid doses and non-opioids. No opioid policy research to date has accounted for this two-pronged approach in their research design. We develop a theory of physician prescribing behavior under this two-pronged incentive structure. Using the Medical Expenditure Panel Survey, we empirically corroborate the theory: regulations and guidelines have the intended effects of reducing opioid prescriptions for acute and chronic pain, respectively, as well as the predicted unintended effects-income effects cause regulations on acute pain treatment to increase chronic pain opioid prescriptions and the chronic pain treatment guidelines spillover to reduce opioids for acute pain. Moreover, we find that the guidelines worked as intended in terms of the reduced usage, with chronic pain patients shifting to non-opioids and also tapering opioid doses. For those who discontinued opioids under regulations and guidelines, we find no harm in terms of increased work limitations due to pain a year after discontinuing opioids. Finally, we observe an unexplained dichotomy-regulations reduce opioid use by causing fewer new starts, whereas guidelines reduce opioid use by discontinuing current users, with no impact on new starts.
期刊介绍:
The focus of the International Journal of Health Economics and Management is on health care systems and on the behavior of consumers, patients, and providers of such services. The links among management, public policy, payment, and performance are core topics of the relaunched journal. The demand for health care and its cost remain central concerns. Even as medical innovation allows providers to improve the lives of their patients, questions remain about how to efficiently deliver health care services, how to pay for it, and who should pay for it. These are central questions facing innovators, providers, and payers in the public and private sectors. One key to answering these questions is to understand how people choose among alternative arrangements, either in markets or through the political process. The choices made by healthcare managers concerning the organization and production of that care are also crucial. There is an important connection between the management of a health care system and its economic performance. The primary audience for this journal will be health economists and researchers in health management, along with the larger group of health services researchers. In addition, research and policy analysis reported in the journal should be of interest to health care providers, managers and policymakers, who need to know about the pressures facing insurers and governments, with consequences for regulation and mandates. The editors of the journal encourage submissions that analyze the behavior and interaction of the actors in health care, viz. consumers, providers, insurers, and governments. Preference will be given to contributions that combine theoretical with empirical work, evaluate conflicting findings, present new information, or compare experiences between countries and jurisdictions. In addition to conventional research articles, the journal will include specific subsections for shorter concise research findings and cont ributions to management and policy that provide important descriptive data or arguments about what policies follow from research findings. The composition of the editorial board is designed to cover the range of interest among economics and management researchers.Officially cited as: Int J Health Econ ManagFrom 2001 to 2014 the journal was published as International Journal of Health Care Finance and Economics. (Articles published in Vol. 1-14 officially cited as: Int J Health Care Finance Econ)



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
