Oluwatobi O Onafowokan, Aboubakr Khairat, Mohammad Jamal, Hemant Chatrath, Hugo J R Bonatti
{"title":"纵向胃切除术治疗非减肥适应症。","authors":"Oluwatobi O Onafowokan, Aboubakr Khairat, Mohammad Jamal, Hemant Chatrath, Hugo J R Bonatti","doi":"10.1155/2021/9962130","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sleeve gastrectomy is the most commonly performed bariatric procedure. Laparoscopic longitudinal gastrectomy (LLG) may be indicated for other indications. <i>Patients and Methods</i>. Two men and two women aged 67, 72, 77, and 80 years underwent LLG for nonbariatric indications with two having normal weight, one being cachectic, and one severely obese.</p><p><strong>Results: </strong>LLG was discussed with patients prior to surgery, but decision for LLG was made during surgery after contemplating other surgical options. A wide sleeve over a 42 French bougie was created with the staple line being oversewn with running 3-0 silk. Indications included a bleeding Dieulafoy lesion that failed endoscopic clipping, fundus gland polyposis found during paraesophageal hernia repair, fundus nodules suspected to be leiomyosarcoma metastases revealing splenosis on final pathology, and significant gastric dilatation associated with organoaxial gastric volvulus. Three patients had an uneventful recovery; the severely obese patient temporarily lost weight but died after two years from a stroke. The last patient developed dysphagia due to an alpha-loop in the sleeve, which was managed by endoscopic stenting. The device subsequently migrated and was laparoscopically removed, with a side-side gastrogastrostomy performed to straighten the alpha-loop. The patient tolerated food better and with overnight PEG tube feeds gained weight but continued heavy smoking. He died after one year from COPD exacerbation.</p><p><strong>Conclusion: </strong>LLG seems to be an appropriate intervention for various gastric pathologies. Training of residents and fellows in the minimally invasive surgical steps of LLG is encouraged.</p>","PeriodicalId":45110,"journal":{"name":"Minimally Invasive Surgery","volume":"2021 ","pages":"9962130"},"PeriodicalIF":1.3000,"publicationDate":"2021-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8124009/pdf/","citationCount":"0","resultStr":"{\"title\":\"Longitudinal Gastrectomy for Nonbariatric Indications.\",\"authors\":\"Oluwatobi O Onafowokan, Aboubakr Khairat, Mohammad Jamal, Hemant Chatrath, Hugo J R Bonatti\",\"doi\":\"10.1155/2021/9962130\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sleeve gastrectomy is the most commonly performed bariatric procedure. Laparoscopic longitudinal gastrectomy (LLG) may be indicated for other indications. <i>Patients and Methods</i>. Two men and two women aged 67, 72, 77, and 80 years underwent LLG for nonbariatric indications with two having normal weight, one being cachectic, and one severely obese.</p><p><strong>Results: </strong>LLG was discussed with patients prior to surgery, but decision for LLG was made during surgery after contemplating other surgical options. A wide sleeve over a 42 French bougie was created with the staple line being oversewn with running 3-0 silk. Indications included a bleeding Dieulafoy lesion that failed endoscopic clipping, fundus gland polyposis found during paraesophageal hernia repair, fundus nodules suspected to be leiomyosarcoma metastases revealing splenosis on final pathology, and significant gastric dilatation associated with organoaxial gastric volvulus. Three patients had an uneventful recovery; the severely obese patient temporarily lost weight but died after two years from a stroke. The last patient developed dysphagia due to an alpha-loop in the sleeve, which was managed by endoscopic stenting. The device subsequently migrated and was laparoscopically removed, with a side-side gastrogastrostomy performed to straighten the alpha-loop. The patient tolerated food better and with overnight PEG tube feeds gained weight but continued heavy smoking. He died after one year from COPD exacerbation.</p><p><strong>Conclusion: </strong>LLG seems to be an appropriate intervention for various gastric pathologies. Training of residents and fellows in the minimally invasive surgical steps of LLG is encouraged.</p>\",\"PeriodicalId\":45110,\"journal\":{\"name\":\"Minimally Invasive Surgery\",\"volume\":\"2021 \",\"pages\":\"9962130\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2021-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8124009/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Minimally Invasive Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/9962130\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Minimally Invasive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/9962130","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Longitudinal Gastrectomy for Nonbariatric Indications.
Background: Sleeve gastrectomy is the most commonly performed bariatric procedure. Laparoscopic longitudinal gastrectomy (LLG) may be indicated for other indications. Patients and Methods. Two men and two women aged 67, 72, 77, and 80 years underwent LLG for nonbariatric indications with two having normal weight, one being cachectic, and one severely obese.
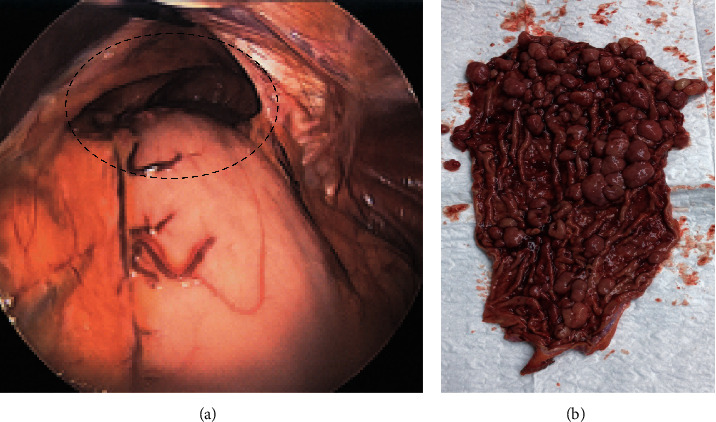
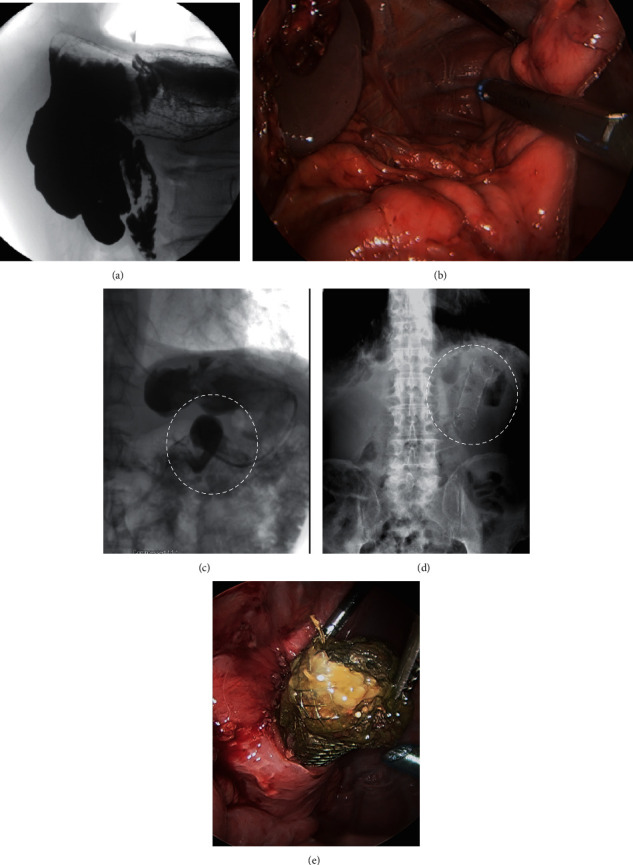
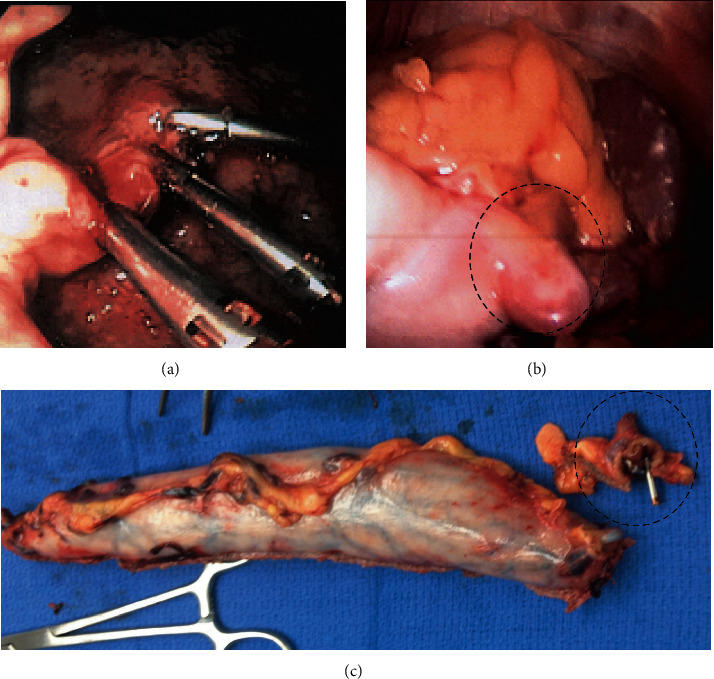
Results: LLG was discussed with patients prior to surgery, but decision for LLG was made during surgery after contemplating other surgical options. A wide sleeve over a 42 French bougie was created with the staple line being oversewn with running 3-0 silk. Indications included a bleeding Dieulafoy lesion that failed endoscopic clipping, fundus gland polyposis found during paraesophageal hernia repair, fundus nodules suspected to be leiomyosarcoma metastases revealing splenosis on final pathology, and significant gastric dilatation associated with organoaxial gastric volvulus. Three patients had an uneventful recovery; the severely obese patient temporarily lost weight but died after two years from a stroke. The last patient developed dysphagia due to an alpha-loop in the sleeve, which was managed by endoscopic stenting. The device subsequently migrated and was laparoscopically removed, with a side-side gastrogastrostomy performed to straighten the alpha-loop. The patient tolerated food better and with overnight PEG tube feeds gained weight but continued heavy smoking. He died after one year from COPD exacerbation.
Conclusion: LLG seems to be an appropriate intervention for various gastric pathologies. Training of residents and fellows in the minimally invasive surgical steps of LLG is encouraged.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
