Katrin Bauer, Frank Heinzelmann, Robert Vogel, Peter Büchler, Björn Mück
{"title":"腹膜透析患者复发性脐疝的机器人辅助增强视野全腹膜外修复(eTEP)","authors":"Katrin Bauer, Frank Heinzelmann, Robert Vogel, Peter Büchler, Björn Mück","doi":"10.3205/iprs000158","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Abdominal wall hernias are frequent in patients with peritoneal dialysis. Guidelines recommend an open hernia repair with extraperitoneal mesh placement to avoid access to the abdominal cavity. <b>Method:</b> We performed a lateral docking robotically assisted enhanced-view totally extraperitoneal repair (eTEP) of a recurrent umbilical hernia with diastasis recti in a patient with peritoneal dialysis due to polycystic kidney disease. After suturing of the midline a 20 x 28 cm mesh was placed in the retrorectus space, covering the whole area of preparation while also overlapping all trocar sites. A drainage was left in the retrorectus space until the first session of PD did not sample any form of leakage. <b>Result:</b> Robotically assisted totally extraperitoneal hernia repair was feasible. The patient was able to continue peritoneal dialysis without intermittent hemodialysis. There was no leakage of the dialysate to the retrorectus space. Postoperative recovery was uneventful. 6 months after surgery the patient was free from pain and showed no signs of recurrence. <b>Conclusion:</b> Robotically assisted totally extraperitoneal hernia repair in patients with umbilical hernia and peritoneal dialysis could be a promising surgical technique to combine the advantages of minimally-invasive surgery with totally extraperitoneal mesh placement without access to the abdominal cavity.</p>","PeriodicalId":43347,"journal":{"name":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","volume":"10 ","pages":"Doc08"},"PeriodicalIF":1.5000,"publicationDate":"2021-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8204666/pdf/","citationCount":"0","resultStr":"{\"title\":\"Robotically assisted enhanced-view totally extraperitoneal repair (eTEP) of a recurrent umbilical hernia in a patient with peritoneal dialysis.\",\"authors\":\"Katrin Bauer, Frank Heinzelmann, Robert Vogel, Peter Büchler, Björn Mück\",\"doi\":\"10.3205/iprs000158\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Abdominal wall hernias are frequent in patients with peritoneal dialysis. Guidelines recommend an open hernia repair with extraperitoneal mesh placement to avoid access to the abdominal cavity. <b>Method:</b> We performed a lateral docking robotically assisted enhanced-view totally extraperitoneal repair (eTEP) of a recurrent umbilical hernia with diastasis recti in a patient with peritoneal dialysis due to polycystic kidney disease. After suturing of the midline a 20 x 28 cm mesh was placed in the retrorectus space, covering the whole area of preparation while also overlapping all trocar sites. A drainage was left in the retrorectus space until the first session of PD did not sample any form of leakage. <b>Result:</b> Robotically assisted totally extraperitoneal hernia repair was feasible. The patient was able to continue peritoneal dialysis without intermittent hemodialysis. There was no leakage of the dialysate to the retrorectus space. Postoperative recovery was uneventful. 6 months after surgery the patient was free from pain and showed no signs of recurrence. <b>Conclusion:</b> Robotically assisted totally extraperitoneal hernia repair in patients with umbilical hernia and peritoneal dialysis could be a promising surgical technique to combine the advantages of minimally-invasive surgery with totally extraperitoneal mesh placement without access to the abdominal cavity.</p>\",\"PeriodicalId\":43347,\"journal\":{\"name\":\"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW\",\"volume\":\"10 \",\"pages\":\"Doc08\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2021-06-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8204666/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3205/iprs000158\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/iprs000158","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
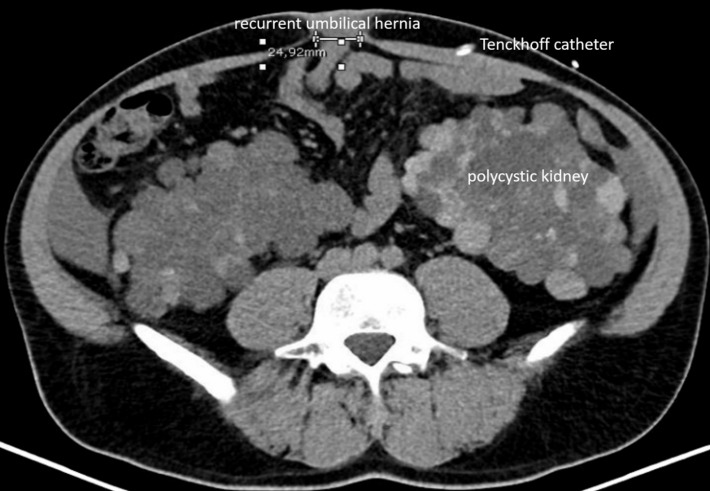
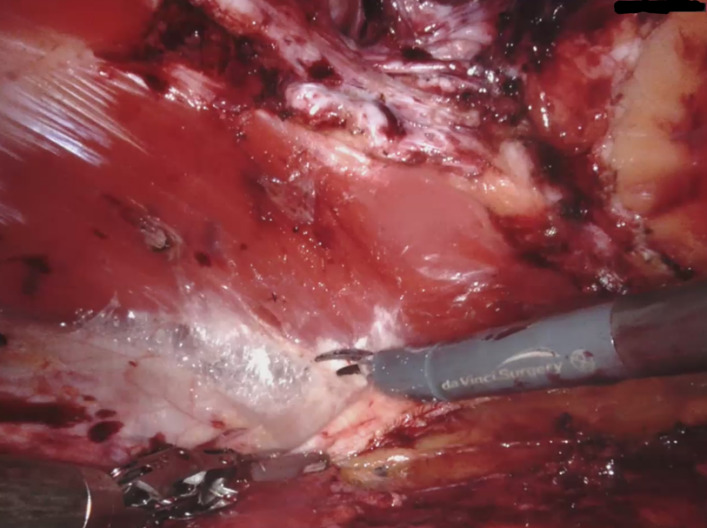
背景:腹膜透析患者常发生腹壁疝。指南推荐开放式疝修补术,腹膜外放置补片以避免进入腹腔。方法:我们对一例多囊肾病腹膜透析的复发性脐疝进行了机器人辅助增强视野全腹膜外修复术(eTEP)。缝合中线后,在直肌间隙放置一个20 x 28 cm的网片,覆盖整个准备区域,同时重叠所有套管针部位。在第一次PD检查没有发现任何形式的渗漏之前,将引流液留在直肌间隙。结果:机器人辅助全腹膜外疝修补术是可行的。患者能够继续腹膜透析而无需间歇血液透析。透析液未渗漏至直肌间隙。术后恢复顺利。术后6个月患者无疼痛,无复发迹象。结论:机器人辅助全腹膜外疝修复脐疝腹膜透析患者是一种很有前途的手术技术,它结合了微创手术和不进入腹腔的全腹膜外补片置入的优点。
Robotically assisted enhanced-view totally extraperitoneal repair (eTEP) of a recurrent umbilical hernia in a patient with peritoneal dialysis.
Background: Abdominal wall hernias are frequent in patients with peritoneal dialysis. Guidelines recommend an open hernia repair with extraperitoneal mesh placement to avoid access to the abdominal cavity. Method: We performed a lateral docking robotically assisted enhanced-view totally extraperitoneal repair (eTEP) of a recurrent umbilical hernia with diastasis recti in a patient with peritoneal dialysis due to polycystic kidney disease. After suturing of the midline a 20 x 28 cm mesh was placed in the retrorectus space, covering the whole area of preparation while also overlapping all trocar sites. A drainage was left in the retrorectus space until the first session of PD did not sample any form of leakage. Result: Robotically assisted totally extraperitoneal hernia repair was feasible. The patient was able to continue peritoneal dialysis without intermittent hemodialysis. There was no leakage of the dialysate to the retrorectus space. Postoperative recovery was uneventful. 6 months after surgery the patient was free from pain and showed no signs of recurrence. Conclusion: Robotically assisted totally extraperitoneal hernia repair in patients with umbilical hernia and peritoneal dialysis could be a promising surgical technique to combine the advantages of minimally-invasive surgery with totally extraperitoneal mesh placement without access to the abdominal cavity.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
