Julius Tetens Hald, Anne Brun Hesselvig, Andreas Kryger Jensen, Anders Odgaard
{"title":"全国全膝关节置换术患者和单室膝关节置换术患者手术季节性分层假体周围关节感染率的修订:一项基于登记的分析。","authors":"Julius Tetens Hald, Anne Brun Hesselvig, Andreas Kryger Jensen, Anders Odgaard","doi":"10.5194/jbji-6-111-2021","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim</b>: The aim of this study was to investigate whether the revision rate for periprosthetic joint infection (PJI) depends on the season of the primary procedure using a national population of knee arthroplasty (KA) patients. Seasonal variation of some surgical procedures has been observed to impact subsequent infection risks, with a higher risk of revision for surgeries performed during summer, but an analysis of PJI rates based on a national arthroplasty register has yet to be completed. We hypothesized that an increased risk of revision due to PJI could be demonstrated in a national population when primary surgery was performed during the summer. <b>Methods</b>: The Danish Knee Arthroplasty Registry (DKR) was used to determine the risk of revision due to PJI within 2 years after primary surgery. All primary KA procedures between 1 January 1997 and 31 December 2014 and revisions until 31 December 2016 were identified. Smoothing spline regression was used to identify possible seasonal pattern effects of the primary procedure on revision risk, and logistic regression was used to calculate risk of infection differences between seasons. <b>Results</b>: A total number of 124 809 primary procedures was registered in the study period. After excluding duplicates and matching primary procedures with the first revisions within 2 years after the primary procedure, 3391 were identified. Of these, 348 cases were recorded with an indication of deep infection requiring revision. Spline regression analyses did not demonstrate any clear seasonal pattern of the primary procedure regarding the risk of revision for infection or any other cause. Logistic regression found a decreased risk of revision for infection when the primary procedure was performed during the summer in the years 1997 to 2005, no influence on the risk of revision for infection in 2005 to 2012, and an increased risk of revision for infection following summer procedures during the years 2013 to 2014. <b>Conclusion</b>: It was not possible to demonstrate a consistent seasonal variation of the risk of revision for PJI following primary KA. This is most likely because the underlying etiologies for PJI are not subject to seasonal variation.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"6 5","pages":"111-117"},"PeriodicalIF":2.8000,"publicationDate":"2021-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8129906/pdf/","citationCount":"2","resultStr":"{\"title\":\"Revision for periprosthetic joint infection rate stratified by seasonality of operation in a national population of total and unicompartmental knee arthroplasty patients: a register-based analysis.\",\"authors\":\"Julius Tetens Hald, Anne Brun Hesselvig, Andreas Kryger Jensen, Anders Odgaard\",\"doi\":\"10.5194/jbji-6-111-2021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Aim</b>: The aim of this study was to investigate whether the revision rate for periprosthetic joint infection (PJI) depends on the season of the primary procedure using a national population of knee arthroplasty (KA) patients. Seasonal variation of some surgical procedures has been observed to impact subsequent infection risks, with a higher risk of revision for surgeries performed during summer, but an analysis of PJI rates based on a national arthroplasty register has yet to be completed. We hypothesized that an increased risk of revision due to PJI could be demonstrated in a national population when primary surgery was performed during the summer. <b>Methods</b>: The Danish Knee Arthroplasty Registry (DKR) was used to determine the risk of revision due to PJI within 2 years after primary surgery. All primary KA procedures between 1 January 1997 and 31 December 2014 and revisions until 31 December 2016 were identified. Smoothing spline regression was used to identify possible seasonal pattern effects of the primary procedure on revision risk, and logistic regression was used to calculate risk of infection differences between seasons. <b>Results</b>: A total number of 124 809 primary procedures was registered in the study period. After excluding duplicates and matching primary procedures with the first revisions within 2 years after the primary procedure, 3391 were identified. Of these, 348 cases were recorded with an indication of deep infection requiring revision. Spline regression analyses did not demonstrate any clear seasonal pattern of the primary procedure regarding the risk of revision for infection or any other cause. Logistic regression found a decreased risk of revision for infection when the primary procedure was performed during the summer in the years 1997 to 2005, no influence on the risk of revision for infection in 2005 to 2012, and an increased risk of revision for infection following summer procedures during the years 2013 to 2014. <b>Conclusion</b>: It was not possible to demonstrate a consistent seasonal variation of the risk of revision for PJI following primary KA. This is most likely because the underlying etiologies for PJI are not subject to seasonal variation.</p>\",\"PeriodicalId\":15271,\"journal\":{\"name\":\"Journal of Bone and Joint Infection\",\"volume\":\"6 5\",\"pages\":\"111-117\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2021-03-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8129906/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Bone and Joint Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5194/jbji-6-111-2021\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-6-111-2021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Revision for periprosthetic joint infection rate stratified by seasonality of operation in a national population of total and unicompartmental knee arthroplasty patients: a register-based analysis.
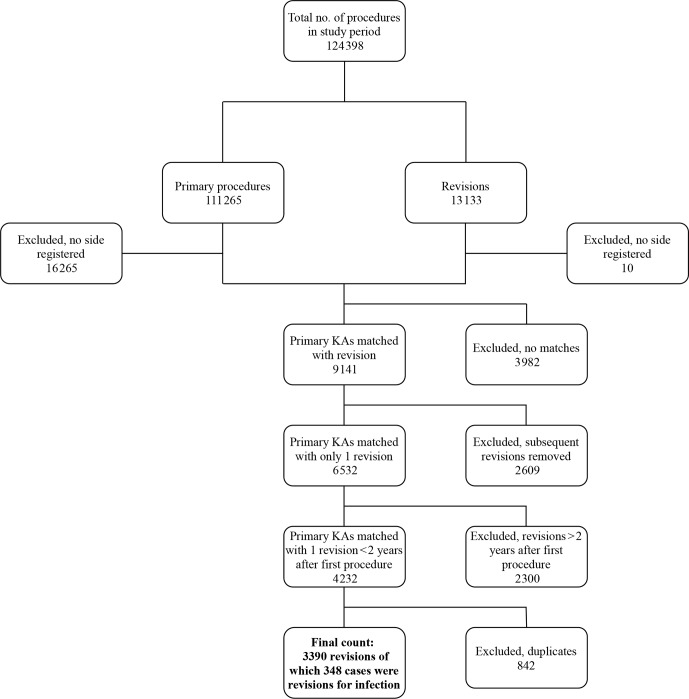
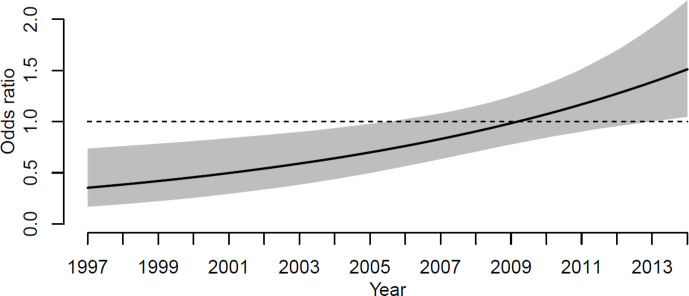
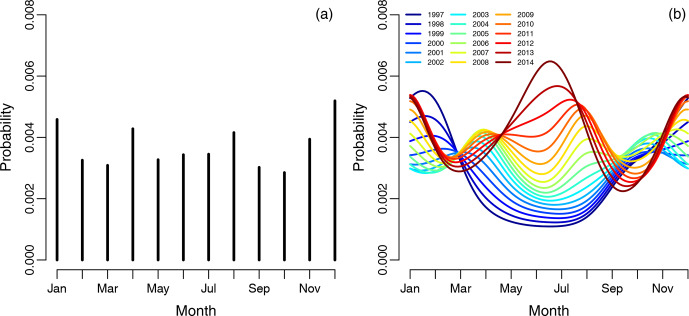
Aim: The aim of this study was to investigate whether the revision rate for periprosthetic joint infection (PJI) depends on the season of the primary procedure using a national population of knee arthroplasty (KA) patients. Seasonal variation of some surgical procedures has been observed to impact subsequent infection risks, with a higher risk of revision for surgeries performed during summer, but an analysis of PJI rates based on a national arthroplasty register has yet to be completed. We hypothesized that an increased risk of revision due to PJI could be demonstrated in a national population when primary surgery was performed during the summer. Methods: The Danish Knee Arthroplasty Registry (DKR) was used to determine the risk of revision due to PJI within 2 years after primary surgery. All primary KA procedures between 1 January 1997 and 31 December 2014 and revisions until 31 December 2016 were identified. Smoothing spline regression was used to identify possible seasonal pattern effects of the primary procedure on revision risk, and logistic regression was used to calculate risk of infection differences between seasons. Results: A total number of 124 809 primary procedures was registered in the study period. After excluding duplicates and matching primary procedures with the first revisions within 2 years after the primary procedure, 3391 were identified. Of these, 348 cases were recorded with an indication of deep infection requiring revision. Spline regression analyses did not demonstrate any clear seasonal pattern of the primary procedure regarding the risk of revision for infection or any other cause. Logistic regression found a decreased risk of revision for infection when the primary procedure was performed during the summer in the years 1997 to 2005, no influence on the risk of revision for infection in 2005 to 2012, and an increased risk of revision for infection following summer procedures during the years 2013 to 2014. Conclusion: It was not possible to demonstrate a consistent seasonal variation of the risk of revision for PJI following primary KA. This is most likely because the underlying etiologies for PJI are not subject to seasonal variation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
