Ravi Saravanan, Rajagopalan Venkatraman, Urkavalan Karthika
{"title":"超声引导改良BRILMA阻滞与肋下经腹平面阻滞用于腹腔镜胆囊切除术术后镇痛的比较——一项随机对照试验。","authors":"Ravi Saravanan, Rajagopalan Venkatraman, Urkavalan Karthika","doi":"10.2147/LRA.S316320","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Subcostal Transversus Abdominis Plane (TAP) block is the standard practice for postoperative analgesia following laparoscopic cholecystectomy. This study aimed to compare the efficacy of modified BRILMA Block (blocking the BRanches of Intercostal nerves at the Level of Mid-Axillary line) with Subcostal TAP block for pain relief following laparoscopic cholecystectomy.</p><p><strong>Methods: </strong>Sixty cases scheduled for laparoscopic cholecystectomy were randomly divided into two groups: modified BRILMA block (Group B) and Subcostal TAP block (Group T). General anesthesia was standardized for both groups. Blocks were performed with 20 mL of 0.2% Ropivacaine under ultrasound guidance after induction of anesthesia. Patients were administered morphine through patient controlled analgesia (PCA) pump with a bolus dose of 1 mg, 10 min lockout interval, and a basal infusion rate of 0.1 mg/h. The pain was assessed by the Visual Analog Scale (VAS) scores of one to ten. The total morphine consumption, time to first request for rescue analgesia, and VAS scores at rest and with movement, and complications, if any, were recorded.</p><p><strong>Results: </strong>The morphine consumption in Group B was 5.67 ± 1.98 mg and in Group T was 5.17 ± 1.85 mg, which was found to be statistically insignificant (p-value = 0.317). The time to first request for rescue analgesia was 759.33 ± 80.29 min in Group B which was comparable to 854 ± 93.01 min in Group T and statistically insignificant (p-value = 0.295). The average VAS scores at rest as well as on movement were comparable in both the groups during the entire 24 h postoperative period. No complications were encountered in our study.</p><p><strong>Conclusion: </strong>Ultrasound-guided modified BRILMA block is equally efficacious as subcostal TAP block in providing postoperative analgesia with similar morphine consumption and no significant difference in VAS scores at rest and movement following laparoscopic cholecystectomy.</p><p><strong>Trial registration number: </strong>CTRI/2020/02/023457.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"14 ","pages":"109-116"},"PeriodicalIF":1.9000,"publicationDate":"2021-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/5c/lra-14-109.PMC8259940.pdf","citationCount":"2","resultStr":"{\"title\":\"Comparison of Ultrasound-Guided Modified BRILMA Block with Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia in Laparoscopic Cholecystectomy - A Randomized Controlled Trial.\",\"authors\":\"Ravi Saravanan, Rajagopalan Venkatraman, Urkavalan Karthika\",\"doi\":\"10.2147/LRA.S316320\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and aims: </strong>Subcostal Transversus Abdominis Plane (TAP) block is the standard practice for postoperative analgesia following laparoscopic cholecystectomy. This study aimed to compare the efficacy of modified BRILMA Block (blocking the BRanches of Intercostal nerves at the Level of Mid-Axillary line) with Subcostal TAP block for pain relief following laparoscopic cholecystectomy.</p><p><strong>Methods: </strong>Sixty cases scheduled for laparoscopic cholecystectomy were randomly divided into two groups: modified BRILMA block (Group B) and Subcostal TAP block (Group T). General anesthesia was standardized for both groups. Blocks were performed with 20 mL of 0.2% Ropivacaine under ultrasound guidance after induction of anesthesia. Patients were administered morphine through patient controlled analgesia (PCA) pump with a bolus dose of 1 mg, 10 min lockout interval, and a basal infusion rate of 0.1 mg/h. The pain was assessed by the Visual Analog Scale (VAS) scores of one to ten. The total morphine consumption, time to first request for rescue analgesia, and VAS scores at rest and with movement, and complications, if any, were recorded.</p><p><strong>Results: </strong>The morphine consumption in Group B was 5.67 ± 1.98 mg and in Group T was 5.17 ± 1.85 mg, which was found to be statistically insignificant (p-value = 0.317). The time to first request for rescue analgesia was 759.33 ± 80.29 min in Group B which was comparable to 854 ± 93.01 min in Group T and statistically insignificant (p-value = 0.295). The average VAS scores at rest as well as on movement were comparable in both the groups during the entire 24 h postoperative period. No complications were encountered in our study.</p><p><strong>Conclusion: </strong>Ultrasound-guided modified BRILMA block is equally efficacious as subcostal TAP block in providing postoperative analgesia with similar morphine consumption and no significant difference in VAS scores at rest and movement following laparoscopic cholecystectomy.</p><p><strong>Trial registration number: </strong>CTRI/2020/02/023457.</p>\",\"PeriodicalId\":18203,\"journal\":{\"name\":\"Local and Regional Anesthesia\",\"volume\":\"14 \",\"pages\":\"109-116\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2021-07-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/5c/lra-14-109.PMC8259940.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Local and Regional Anesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LRA.S316320\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S316320","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Comparison of Ultrasound-Guided Modified BRILMA Block with Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia in Laparoscopic Cholecystectomy - A Randomized Controlled Trial.
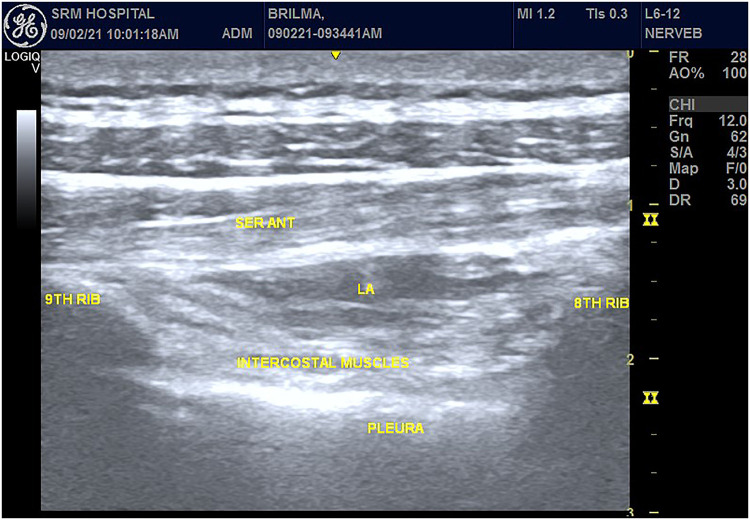
Background and aims: Subcostal Transversus Abdominis Plane (TAP) block is the standard practice for postoperative analgesia following laparoscopic cholecystectomy. This study aimed to compare the efficacy of modified BRILMA Block (blocking the BRanches of Intercostal nerves at the Level of Mid-Axillary line) with Subcostal TAP block for pain relief following laparoscopic cholecystectomy.
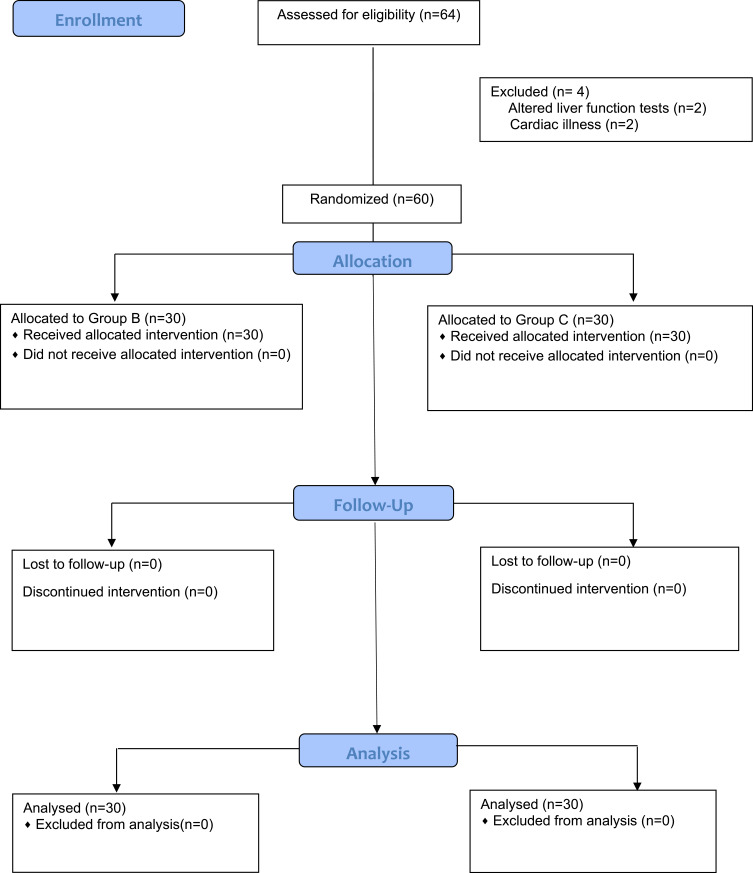
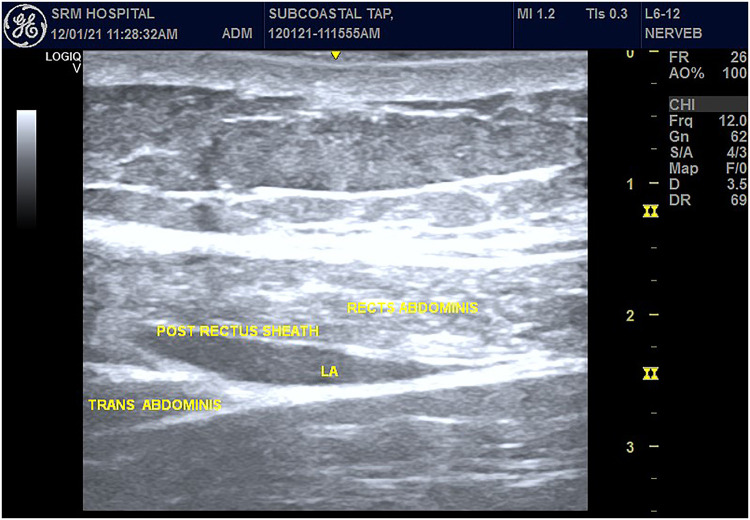
Methods: Sixty cases scheduled for laparoscopic cholecystectomy were randomly divided into two groups: modified BRILMA block (Group B) and Subcostal TAP block (Group T). General anesthesia was standardized for both groups. Blocks were performed with 20 mL of 0.2% Ropivacaine under ultrasound guidance after induction of anesthesia. Patients were administered morphine through patient controlled analgesia (PCA) pump with a bolus dose of 1 mg, 10 min lockout interval, and a basal infusion rate of 0.1 mg/h. The pain was assessed by the Visual Analog Scale (VAS) scores of one to ten. The total morphine consumption, time to first request for rescue analgesia, and VAS scores at rest and with movement, and complications, if any, were recorded.
Results: The morphine consumption in Group B was 5.67 ± 1.98 mg and in Group T was 5.17 ± 1.85 mg, which was found to be statistically insignificant (p-value = 0.317). The time to first request for rescue analgesia was 759.33 ± 80.29 min in Group B which was comparable to 854 ± 93.01 min in Group T and statistically insignificant (p-value = 0.295). The average VAS scores at rest as well as on movement were comparable in both the groups during the entire 24 h postoperative period. No complications were encountered in our study.
Conclusion: Ultrasound-guided modified BRILMA block is equally efficacious as subcostal TAP block in providing postoperative analgesia with similar morphine consumption and no significant difference in VAS scores at rest and movement following laparoscopic cholecystectomy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
