Adaeze C Ayuk, Chizalu I Ndukwu, Samuel N Uwaezuoke
{"title":"在高度有效的抗逆转录病毒治疗中,人类免疫缺陷病毒感染儿童的小气道疾病及其可逆性:在非洲环境中的横断面研究。","authors":"Adaeze C Ayuk, Chizalu I Ndukwu, Samuel N Uwaezuoke","doi":"10.4103/atm.ATM_494_20","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung function abnormalities may occur in children with human immunodeficiency virus (HIV) infection. Small-airway disease (SAD) precedes abnormalities in forced expiratory volume in 1 s (FEV <sub>1</sub>).</p><p><strong>Objective: </strong>This study aims to assess the presence and reversibility of SAD in HIV-infected children using the Global Lung Function Initiative standards.</p><p><strong>Methods: </strong>A cross-sectional study was conducted over 6 months at the Paediatric HIV Clinic of the University of Nigeria Teaching Hospital in Enugu, Southeast Nigeria. Eligible consenting children with HIV infection were recruited. Lung function was measured, and the reversibility of FEV<sub>1</sub> and forced vital capacity (FVC) was assessed at 12% while that of forced expiratory flow between 25% and 75% (FEF<sub>25-75</sub>) was assessed at 12%, 15%, and 20%. Predictors of abnormal Z-score values were determined by multivariate linear and logistic regressions. Statistically significant values were set at <i>P</i> < 0.05.</p><p><strong>Results: </strong>The mean Z-score for FEV<sub>1</sub>, FVC, and FEF<sub>25-75</sub> was - 2.19, -1.86, and - 1.60, respectively. Most patients (73%) had abnormal FEV<sub>1</sub>, while 52% had abnormal FEF<sub>25-75</sub>. Significant changes in FEV<sub>1</sub> (<i>P</i> = 0.001) and FEF<sub>25-75</sub> (<i>P</i> < 0.001) occurred after the bronchodilator response (BDR) test. Of the children whose FEV<sub>1</sub> showed positive BDR, 70.9% had low zFEV<sub>1;</sub> 50% had low zFEF<sub>25-75</sub>, while all had low FEV<sub>1.</sub> Nutritional status (Z-score for body mass index) was significantly associated with low FEV<sub>1.</sub></p><p><strong>Conclusions: </strong>Abnormal FEF<sub>25-75</sub> as a marker of SAD and FEV<sub>1</sub> with a positive BDR are common in HIV-infected children. These lung function abnormalities justify long-term follow-up for these patients.</p>","PeriodicalId":50760,"journal":{"name":"Annals of Thoracic Medicine","volume":"16 3","pages":"253-259"},"PeriodicalIF":2.3000,"publicationDate":"2021-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d6/45/ATM-16-253.PMC8388566.pdf","citationCount":"1","resultStr":"{\"title\":\"Small-airway disease and its reversibility in human immunodeficiency virus-infected children on highly active antiretroviral therapy: A cross-sectional study in an African setting.\",\"authors\":\"Adaeze C Ayuk, Chizalu I Ndukwu, Samuel N Uwaezuoke\",\"doi\":\"10.4103/atm.ATM_494_20\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lung function abnormalities may occur in children with human immunodeficiency virus (HIV) infection. Small-airway disease (SAD) precedes abnormalities in forced expiratory volume in 1 s (FEV <sub>1</sub>).</p><p><strong>Objective: </strong>This study aims to assess the presence and reversibility of SAD in HIV-infected children using the Global Lung Function Initiative standards.</p><p><strong>Methods: </strong>A cross-sectional study was conducted over 6 months at the Paediatric HIV Clinic of the University of Nigeria Teaching Hospital in Enugu, Southeast Nigeria. Eligible consenting children with HIV infection were recruited. Lung function was measured, and the reversibility of FEV<sub>1</sub> and forced vital capacity (FVC) was assessed at 12% while that of forced expiratory flow between 25% and 75% (FEF<sub>25-75</sub>) was assessed at 12%, 15%, and 20%. Predictors of abnormal Z-score values were determined by multivariate linear and logistic regressions. Statistically significant values were set at <i>P</i> < 0.05.</p><p><strong>Results: </strong>The mean Z-score for FEV<sub>1</sub>, FVC, and FEF<sub>25-75</sub> was - 2.19, -1.86, and - 1.60, respectively. Most patients (73%) had abnormal FEV<sub>1</sub>, while 52% had abnormal FEF<sub>25-75</sub>. Significant changes in FEV<sub>1</sub> (<i>P</i> = 0.001) and FEF<sub>25-75</sub> (<i>P</i> < 0.001) occurred after the bronchodilator response (BDR) test. Of the children whose FEV<sub>1</sub> showed positive BDR, 70.9% had low zFEV<sub>1;</sub> 50% had low zFEF<sub>25-75</sub>, while all had low FEV<sub>1.</sub> Nutritional status (Z-score for body mass index) was significantly associated with low FEV<sub>1.</sub></p><p><strong>Conclusions: </strong>Abnormal FEF<sub>25-75</sub> as a marker of SAD and FEV<sub>1</sub> with a positive BDR are common in HIV-infected children. These lung function abnormalities justify long-term follow-up for these patients.</p>\",\"PeriodicalId\":50760,\"journal\":{\"name\":\"Annals of Thoracic Medicine\",\"volume\":\"16 3\",\"pages\":\"253-259\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2021-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d6/45/ATM-16-253.PMC8388566.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4103/atm.ATM_494_20\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/7/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/atm.ATM_494_20","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/7/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Small-airway disease and its reversibility in human immunodeficiency virus-infected children on highly active antiretroviral therapy: A cross-sectional study in an African setting.
Background: Lung function abnormalities may occur in children with human immunodeficiency virus (HIV) infection. Small-airway disease (SAD) precedes abnormalities in forced expiratory volume in 1 s (FEV 1).
Objective: This study aims to assess the presence and reversibility of SAD in HIV-infected children using the Global Lung Function Initiative standards.
Methods: A cross-sectional study was conducted over 6 months at the Paediatric HIV Clinic of the University of Nigeria Teaching Hospital in Enugu, Southeast Nigeria. Eligible consenting children with HIV infection were recruited. Lung function was measured, and the reversibility of FEV1 and forced vital capacity (FVC) was assessed at 12% while that of forced expiratory flow between 25% and 75% (FEF25-75) was assessed at 12%, 15%, and 20%. Predictors of abnormal Z-score values were determined by multivariate linear and logistic regressions. Statistically significant values were set at P < 0.05.
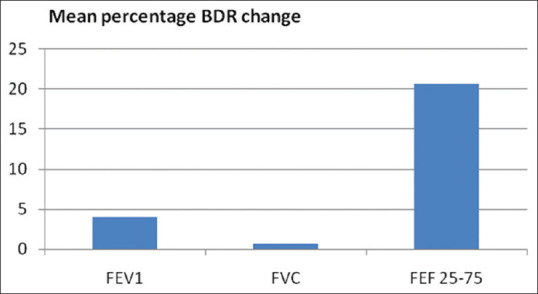
Results: The mean Z-score for FEV1, FVC, and FEF25-75 was - 2.19, -1.86, and - 1.60, respectively. Most patients (73%) had abnormal FEV1, while 52% had abnormal FEF25-75. Significant changes in FEV1 (P = 0.001) and FEF25-75 (P < 0.001) occurred after the bronchodilator response (BDR) test. Of the children whose FEV1 showed positive BDR, 70.9% had low zFEV1; 50% had low zFEF25-75, while all had low FEV1. Nutritional status (Z-score for body mass index) was significantly associated with low FEV1.
Conclusions: Abnormal FEF25-75 as a marker of SAD and FEV1 with a positive BDR are common in HIV-infected children. These lung function abnormalities justify long-term follow-up for these patients.
期刊介绍:
The journal will cover studies related to multidisciplinary specialties of chest medicine, such as adult and pediatrics pulmonology, thoracic surgery, critical care medicine, respiratory care, transplantation, sleep medicine, related basic medical sciences, and more. The journal also features basic science, special reports, case reports, board review , and more. Editorials and communications to the editor that explore controversial issues and encourage further discussion by physicians dealing with chest medicine.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
