Joke Delvaux, Alexandra John, Lucy Wedderburn, Jacqui Morris
{"title":"在卒中随机对照可行性试验的背景下实施动态Lycra®矫形器进行手臂康复:一项使用归一化过程理论的定性研究。","authors":"Joke Delvaux, Alexandra John, Lucy Wedderburn, Jacqui Morris","doi":"10.1177/1179572720950210","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To explore how non-research funded rehabilitation practitioners implemented dynamic Lycra<sup>®</sup> orthoses for arm recovery after stroke into rehabilitation practice, as part of a feasibility randomised controlled trial.</p><p><strong>Design: </strong>Qualitative interview study.</p><p><strong>Setting: </strong>Two in-patient stroke units and associated rehabilitation units.</p><p><strong>Subjects: </strong>Fifteen purposefully selected stroke rehabilitation practitioners involved in delivery of dynamic Lycra<sup>®</sup> orthoses as part of a feasibility randomised controlled trial.</p><p><strong>Methods: </strong>Semi-structured interviews conducted at the end of the trial. Interviews examined their experiences of orthosis implementation. Normalisation Process Theory structured the interview guide and informed data analysis. NVivo software supported data analysis.</p><p><strong>Results: </strong>Practitioners intuitively made sense of the intervention in the face of uncertainty about its precise mechanisms of action (Normalisation Process Theory construct: coherence) and espoused commitment to the research, despite uncertainty about orthosis effectiveness (cognitive participation). They did however adapt the intervention based on perceived therapeutic need, their own skillsets and stroke survivor preference (collective action). They were uncertain about benefits (reflexive monitoring). Across the 4 theoretical constructs, ambivalence about the intervention was detected.</p><p><strong>Conclusions: </strong>Ambivalence interfered with implementation - but only to an extent. 'Good-enough' coherence, cognitive participation, collective action and reflexive monitoring were sufficient to initiate normalisation - as long as implementation did not undermine the relationship between practitioner and stroke survivor. Ambivalence stemmed from practitioners' uncertainty about the intervention theory and mechanisms of action. Making intervention mechanisms of action more explicit to practitioners may influence how they implement and adapt a research intervention, and may determine whether those processes undermine or enhance outcomes.</p>","PeriodicalId":41347,"journal":{"name":"Rehabilitation Process and Outcome","volume":"9 ","pages":"1179572720950210"},"PeriodicalIF":1.4000,"publicationDate":"2020-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179572720950210","citationCount":"3","resultStr":"{\"title\":\"Implementation of Dynamic Lycra<sup>®</sup> Orthoses for Arm Rehabilitation in the Context of a Randomised Controlled Feasibility Trial in Stroke: A Qualitative study Using Normalisation Process Theory.\",\"authors\":\"Joke Delvaux, Alexandra John, Lucy Wedderburn, Jacqui Morris\",\"doi\":\"10.1177/1179572720950210\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To explore how non-research funded rehabilitation practitioners implemented dynamic Lycra<sup>®</sup> orthoses for arm recovery after stroke into rehabilitation practice, as part of a feasibility randomised controlled trial.</p><p><strong>Design: </strong>Qualitative interview study.</p><p><strong>Setting: </strong>Two in-patient stroke units and associated rehabilitation units.</p><p><strong>Subjects: </strong>Fifteen purposefully selected stroke rehabilitation practitioners involved in delivery of dynamic Lycra<sup>®</sup> orthoses as part of a feasibility randomised controlled trial.</p><p><strong>Methods: </strong>Semi-structured interviews conducted at the end of the trial. Interviews examined their experiences of orthosis implementation. Normalisation Process Theory structured the interview guide and informed data analysis. NVivo software supported data analysis.</p><p><strong>Results: </strong>Practitioners intuitively made sense of the intervention in the face of uncertainty about its precise mechanisms of action (Normalisation Process Theory construct: coherence) and espoused commitment to the research, despite uncertainty about orthosis effectiveness (cognitive participation). They did however adapt the intervention based on perceived therapeutic need, their own skillsets and stroke survivor preference (collective action). They were uncertain about benefits (reflexive monitoring). Across the 4 theoretical constructs, ambivalence about the intervention was detected.</p><p><strong>Conclusions: </strong>Ambivalence interfered with implementation - but only to an extent. 'Good-enough' coherence, cognitive participation, collective action and reflexive monitoring were sufficient to initiate normalisation - as long as implementation did not undermine the relationship between practitioner and stroke survivor. Ambivalence stemmed from practitioners' uncertainty about the intervention theory and mechanisms of action. Making intervention mechanisms of action more explicit to practitioners may influence how they implement and adapt a research intervention, and may determine whether those processes undermine or enhance outcomes.</p>\",\"PeriodicalId\":41347,\"journal\":{\"name\":\"Rehabilitation Process and Outcome\",\"volume\":\"9 \",\"pages\":\"1179572720950210\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2020-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179572720950210\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rehabilitation Process and Outcome\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179572720950210\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"REHABILITATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rehabilitation Process and Outcome","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179572720950210","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
Implementation of Dynamic Lycra® Orthoses for Arm Rehabilitation in the Context of a Randomised Controlled Feasibility Trial in Stroke: A Qualitative study Using Normalisation Process Theory.
Objective: To explore how non-research funded rehabilitation practitioners implemented dynamic Lycra® orthoses for arm recovery after stroke into rehabilitation practice, as part of a feasibility randomised controlled trial.
Design: Qualitative interview study.
Setting: Two in-patient stroke units and associated rehabilitation units.
Subjects: Fifteen purposefully selected stroke rehabilitation practitioners involved in delivery of dynamic Lycra® orthoses as part of a feasibility randomised controlled trial.
Methods: Semi-structured interviews conducted at the end of the trial. Interviews examined their experiences of orthosis implementation. Normalisation Process Theory structured the interview guide and informed data analysis. NVivo software supported data analysis.
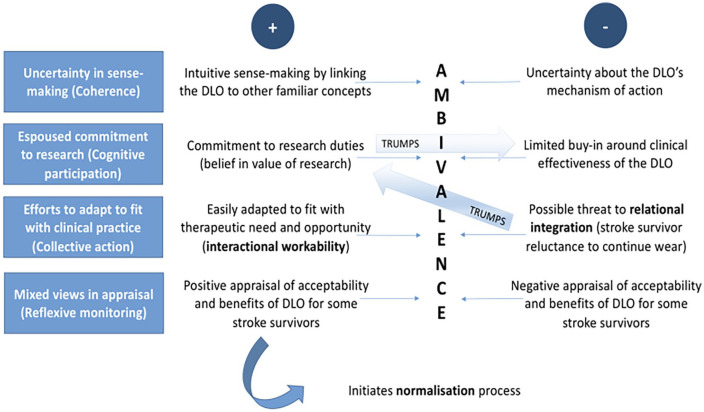
Results: Practitioners intuitively made sense of the intervention in the face of uncertainty about its precise mechanisms of action (Normalisation Process Theory construct: coherence) and espoused commitment to the research, despite uncertainty about orthosis effectiveness (cognitive participation). They did however adapt the intervention based on perceived therapeutic need, their own skillsets and stroke survivor preference (collective action). They were uncertain about benefits (reflexive monitoring). Across the 4 theoretical constructs, ambivalence about the intervention was detected.
Conclusions: Ambivalence interfered with implementation - but only to an extent. 'Good-enough' coherence, cognitive participation, collective action and reflexive monitoring were sufficient to initiate normalisation - as long as implementation did not undermine the relationship between practitioner and stroke survivor. Ambivalence stemmed from practitioners' uncertainty about the intervention theory and mechanisms of action. Making intervention mechanisms of action more explicit to practitioners may influence how they implement and adapt a research intervention, and may determine whether those processes undermine or enhance outcomes.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
