Nikhil V Kotha, Rohith S Voora, Alex S Qian, Abhishek Kumar, Edmund M Qiao, Tyler F Stewart, Brent S Rose, Ryan K Orosco
{"title":"中性粒细胞/淋巴细胞比值预处理在晚期喉癌预后中的应用。","authors":"Nikhil V Kotha, Rohith S Voora, Alex S Qian, Abhishek Kumar, Edmund M Qiao, Tyler F Stewart, Brent S Rose, Ryan K Orosco","doi":"10.1177/11772719211049848","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Neutrophil-lymphocyte ratio has been explored as a prognosticator in several cancer types, but its association with larynx cancer outcomes is not well known. We aimed to identify an optimal NLR cutoff point and examine the prognostic utility of this biomarker in patients with locoregionally advanced larynx cancer treated with curative intent.</p><p><strong>Methods: </strong>In the Veterans Affairs' (VA) national database, we identified patients with locoregionally advanced (T3-4N0-3M0) laryngeal squamous cell carcinoma diagnosed between 2000 and 2017 and treated with curative intent. NLR cutoff points were calculated using Contal/O'Quigley's method. Outcomes of larynx cancer-specific survival (CSS), overall survival (OS), and non-larynx cancer survival (NCS) were evaluated in multivariable Cox and Fine-Gray models.</p><p><strong>Results: </strong>In 1047 patients, the optimal pretreatment NLR cutoff was identified as 4.17 - 722 patients with NLR ⩽ 4.17, 325 patients with NLR > 4.17. The elevated NLR cohort had a higher proportion of T4 disease (39.4% vs 28.4%), node positive disease (52.3% vs 43.1%), and surgical treatment (43.7% vs 35.2%). In multivariable analysis, NLR > 4.17 was independently associated with worse OS (HR 1.31, 95% CI 1.12-1.54, <i>P</i> = .001) and worse CSS (HR 1.46, 95% CI 1.17-1.83, <i>P</i> < .001), but not with NCS (HR 0.94, 95% CI 0.75-1.18, <i>P</i> = .58).</p><p><strong>Conclusion: </strong>In locoregionally advanced larynx cancer treated with curative intent, we identified elevated NLR to be associated with inferior OS and CSS. Further prospective studies are needed to investigate pretreatment NLR and our identified 4.17 cutoff as a potential larynx cancer-specific marker for this high risk population.</p>","PeriodicalId":47060,"journal":{"name":"Biomarker Insights","volume":"16 ","pages":"11772719211049848"},"PeriodicalIF":1.9000,"publicationDate":"2021-10-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/90/02/10.1177_11772719211049848.PMC8512256.pdf","citationCount":"4","resultStr":"{\"title\":\"Prognostic Utility of Pretreatment Neutrophil-Lymphocyte Ratio in Advanced Larynx Cancer.\",\"authors\":\"Nikhil V Kotha, Rohith S Voora, Alex S Qian, Abhishek Kumar, Edmund M Qiao, Tyler F Stewart, Brent S Rose, Ryan K Orosco\",\"doi\":\"10.1177/11772719211049848\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Neutrophil-lymphocyte ratio has been explored as a prognosticator in several cancer types, but its association with larynx cancer outcomes is not well known. We aimed to identify an optimal NLR cutoff point and examine the prognostic utility of this biomarker in patients with locoregionally advanced larynx cancer treated with curative intent.</p><p><strong>Methods: </strong>In the Veterans Affairs' (VA) national database, we identified patients with locoregionally advanced (T3-4N0-3M0) laryngeal squamous cell carcinoma diagnosed between 2000 and 2017 and treated with curative intent. NLR cutoff points were calculated using Contal/O'Quigley's method. Outcomes of larynx cancer-specific survival (CSS), overall survival (OS), and non-larynx cancer survival (NCS) were evaluated in multivariable Cox and Fine-Gray models.</p><p><strong>Results: </strong>In 1047 patients, the optimal pretreatment NLR cutoff was identified as 4.17 - 722 patients with NLR ⩽ 4.17, 325 patients with NLR > 4.17. The elevated NLR cohort had a higher proportion of T4 disease (39.4% vs 28.4%), node positive disease (52.3% vs 43.1%), and surgical treatment (43.7% vs 35.2%). In multivariable analysis, NLR > 4.17 was independently associated with worse OS (HR 1.31, 95% CI 1.12-1.54, <i>P</i> = .001) and worse CSS (HR 1.46, 95% CI 1.17-1.83, <i>P</i> < .001), but not with NCS (HR 0.94, 95% CI 0.75-1.18, <i>P</i> = .58).</p><p><strong>Conclusion: </strong>In locoregionally advanced larynx cancer treated with curative intent, we identified elevated NLR to be associated with inferior OS and CSS. Further prospective studies are needed to investigate pretreatment NLR and our identified 4.17 cutoff as a potential larynx cancer-specific marker for this high risk population.</p>\",\"PeriodicalId\":47060,\"journal\":{\"name\":\"Biomarker Insights\",\"volume\":\"16 \",\"pages\":\"11772719211049848\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2021-10-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/90/02/10.1177_11772719211049848.PMC8512256.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biomarker Insights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11772719211049848\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomarker Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11772719211049848","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 4
摘要
目的:中性粒细胞-淋巴细胞比率已被探讨作为几种癌症类型的预后指标,但其与喉癌预后的关系尚不清楚。我们的目的是确定一个最佳的NLR截止点,并检查该生物标志物在局部区域晚期喉癌患者中治疗意图的预后效用。方法:在退伍军人事务部(VA)国家数据库中,我们确定了2000年至2017年间诊断并以治愈意图治疗的局部晚期(T3-4N0-3M0)喉鳞状细胞癌患者。NLR截止点采用Contal/O'Quigley方法计算。采用多变量Cox和Fine-Gray模型评估喉癌特异性生存期(CSS)、总生存期(OS)和非喉癌生存期(NCS)。结果:1047例患者中,最佳预处理NLR截止值为4.17 ~ 722例NLR≤4.17,325例NLR > 4.17。NLR升高的队列中T4疾病(39.4%比28.4%)、淋巴结阳性疾病(52.3%比43.1%)和手术治疗(43.7%比35.2%)的比例更高。在多变量分析中,NLR > 4.17与较差的OS (HR 1.31, 95% CI 1.12-1.54, P = .001)和较差的CSS (HR 1.46, 95% CI 1.17-1.83, P = .58)独立相关。结论:在以治愈为目的治疗的局部晚期喉癌中,我们发现NLR升高与不良OS和CSS相关。需要进一步的前瞻性研究来调查预处理NLR和我们确定的4.17临界值作为这一高危人群的潜在喉癌特异性标志物。
Prognostic Utility of Pretreatment Neutrophil-Lymphocyte Ratio in Advanced Larynx Cancer.
Purpose: Neutrophil-lymphocyte ratio has been explored as a prognosticator in several cancer types, but its association with larynx cancer outcomes is not well known. We aimed to identify an optimal NLR cutoff point and examine the prognostic utility of this biomarker in patients with locoregionally advanced larynx cancer treated with curative intent.
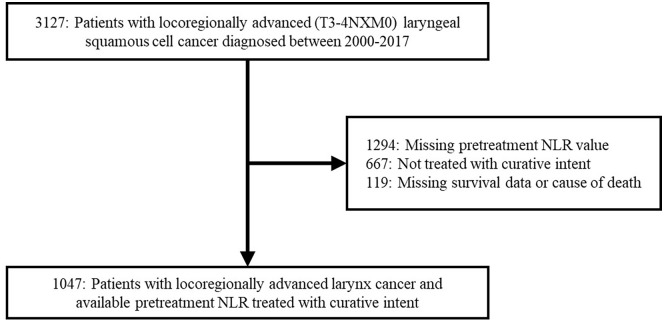
Methods: In the Veterans Affairs' (VA) national database, we identified patients with locoregionally advanced (T3-4N0-3M0) laryngeal squamous cell carcinoma diagnosed between 2000 and 2017 and treated with curative intent. NLR cutoff points were calculated using Contal/O'Quigley's method. Outcomes of larynx cancer-specific survival (CSS), overall survival (OS), and non-larynx cancer survival (NCS) were evaluated in multivariable Cox and Fine-Gray models.
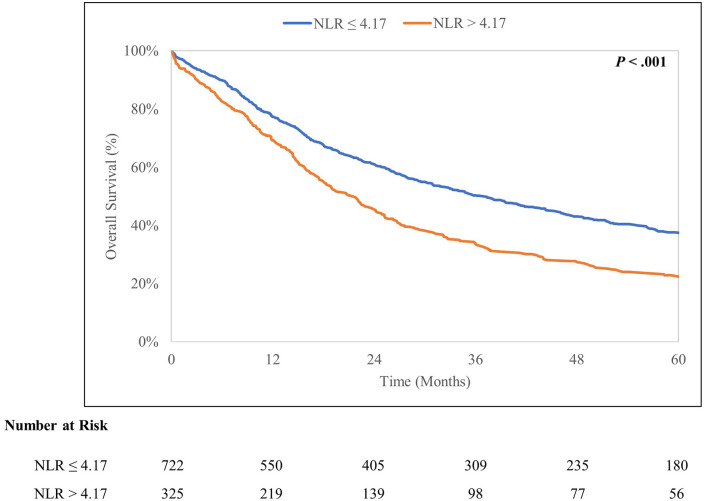
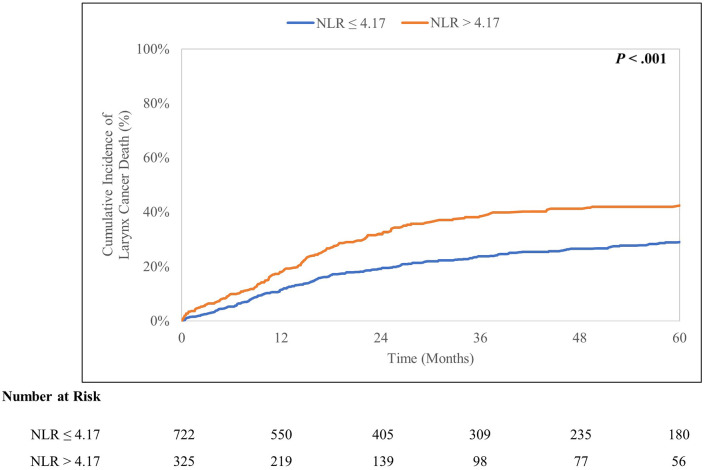
Results: In 1047 patients, the optimal pretreatment NLR cutoff was identified as 4.17 - 722 patients with NLR ⩽ 4.17, 325 patients with NLR > 4.17. The elevated NLR cohort had a higher proportion of T4 disease (39.4% vs 28.4%), node positive disease (52.3% vs 43.1%), and surgical treatment (43.7% vs 35.2%). In multivariable analysis, NLR > 4.17 was independently associated with worse OS (HR 1.31, 95% CI 1.12-1.54, P = .001) and worse CSS (HR 1.46, 95% CI 1.17-1.83, P < .001), but not with NCS (HR 0.94, 95% CI 0.75-1.18, P = .58).
Conclusion: In locoregionally advanced larynx cancer treated with curative intent, we identified elevated NLR to be associated with inferior OS and CSS. Further prospective studies are needed to investigate pretreatment NLR and our identified 4.17 cutoff as a potential larynx cancer-specific marker for this high risk population.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
