Dennis A Eichenauer, Gunnar Lachmann, Paul La Rosée
{"title":"[危重病人的噬血细胞淋巴组织细胞增多症]。","authors":"Dennis A Eichenauer, Gunnar Lachmann, Paul La Rosée","doi":"10.1007/s00740-021-00414-z","DOIUrl":null,"url":null,"abstract":"<p><p>Hemophagocytic lymphohistiocytosis (HLH) is a hyperinflammation syndrome. In adults, secondary HLH is mostly observed. HLH is often triggered by infections, malignancies or autoimmune disorders. However, HLH cases in association with immunotherapies have been described recently. HLH in critically ill patients is often difficult to differentiate from sepsis. Both conditions can also be present at the same time. Early diagnosis and timely initiation of an adequate immunosuppressive therapy are essential for the further course and the prognosis of HLH. Therefore, HLH should represent a differential diagnosis in critically ill patients with persistent fever and additional symptoms (e.g. enlarged spleen, neurologic symptoms) or laboratory parameters (e.g. hyperferritinemia, cytopenia, increased transaminases) compatible with HLH. The diagnosis of HLH is made using the HLH-2004 criteria. The probability of the presence of HLH can be calculated using the HScore. High-dose corticosteroids represent the cornerstone of HLH treatment. Etoposide, immunoglobulins, anakinra or other drugs are added depending on the trigger. The course of HLH is influenced by the time of treatment initiation, the underlying trigger and the response to treatment. Generally, the prognosis of critically ill HLH patients is poor.</p>","PeriodicalId":75323,"journal":{"name":"Wiener klinisches Magazin : Beilage zur Wiener klinischen Wochenschrift","volume":"24 6","pages":"246-251"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8529362/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Hemophagocytic lymphohistiocytosis in critically ill patients].\",\"authors\":\"Dennis A Eichenauer, Gunnar Lachmann, Paul La Rosée\",\"doi\":\"10.1007/s00740-021-00414-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Hemophagocytic lymphohistiocytosis (HLH) is a hyperinflammation syndrome. In adults, secondary HLH is mostly observed. HLH is often triggered by infections, malignancies or autoimmune disorders. However, HLH cases in association with immunotherapies have been described recently. HLH in critically ill patients is often difficult to differentiate from sepsis. Both conditions can also be present at the same time. Early diagnosis and timely initiation of an adequate immunosuppressive therapy are essential for the further course and the prognosis of HLH. Therefore, HLH should represent a differential diagnosis in critically ill patients with persistent fever and additional symptoms (e.g. enlarged spleen, neurologic symptoms) or laboratory parameters (e.g. hyperferritinemia, cytopenia, increased transaminases) compatible with HLH. The diagnosis of HLH is made using the HLH-2004 criteria. The probability of the presence of HLH can be calculated using the HScore. High-dose corticosteroids represent the cornerstone of HLH treatment. Etoposide, immunoglobulins, anakinra or other drugs are added depending on the trigger. The course of HLH is influenced by the time of treatment initiation, the underlying trigger and the response to treatment. Generally, the prognosis of critically ill HLH patients is poor.</p>\",\"PeriodicalId\":75323,\"journal\":{\"name\":\"Wiener klinisches Magazin : Beilage zur Wiener klinischen Wochenschrift\",\"volume\":\"24 6\",\"pages\":\"246-251\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8529362/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Wiener klinisches Magazin : Beilage zur Wiener klinischen Wochenschrift\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s00740-021-00414-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/10/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Wiener klinisches Magazin : Beilage zur Wiener klinischen Wochenschrift","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00740-021-00414-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
[Hemophagocytic lymphohistiocytosis in critically ill patients].
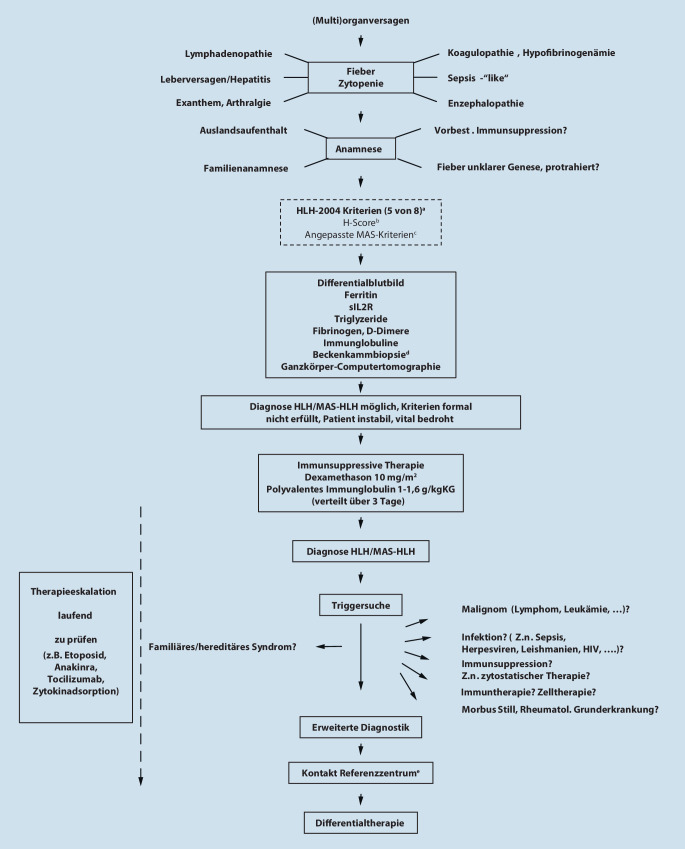
Hemophagocytic lymphohistiocytosis (HLH) is a hyperinflammation syndrome. In adults, secondary HLH is mostly observed. HLH is often triggered by infections, malignancies or autoimmune disorders. However, HLH cases in association with immunotherapies have been described recently. HLH in critically ill patients is often difficult to differentiate from sepsis. Both conditions can also be present at the same time. Early diagnosis and timely initiation of an adequate immunosuppressive therapy are essential for the further course and the prognosis of HLH. Therefore, HLH should represent a differential diagnosis in critically ill patients with persistent fever and additional symptoms (e.g. enlarged spleen, neurologic symptoms) or laboratory parameters (e.g. hyperferritinemia, cytopenia, increased transaminases) compatible with HLH. The diagnosis of HLH is made using the HLH-2004 criteria. The probability of the presence of HLH can be calculated using the HScore. High-dose corticosteroids represent the cornerstone of HLH treatment. Etoposide, immunoglobulins, anakinra or other drugs are added depending on the trigger. The course of HLH is influenced by the time of treatment initiation, the underlying trigger and the response to treatment. Generally, the prognosis of critically ill HLH patients is poor.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
