{"title":"细胞减少手术(CRS)和腹腔热化疗(HIPEC)的术后恢复增强(ERAS):一项横断面调查。","authors":"Geetu Bhandoria, Sohan Lal Solanki, Mrugank Bhavsar, Kalpana Balakrishnan, Cherukuri Bapuji, Nitin Bhorkar, Prashant Bhandarkar, Sameer Bhosale, Jigeeshu V Divatia, Anik Ghosh, Vikas Mahajan, Abraham Peedicayil, Praveen Nath, Snita Sinukumar, Robin Thambudorai, Ramakrishnan Ayloor Seshadri, Aditi Bhatt","doi":"10.1515/pp-2021-0117","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Enhanced recovery after surgery (ERAS) protocols have been questioned in patients undergoing cytoreductive surgery (CRS) with/without hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal malignancies. This survey was performed to study clinicians' practice about ERAS in patients undergoing CRS-HIPEC.</p><p><strong>Methods: </strong>An online survey, comprising 76 questions on elements of prehabilitation (n=11), preoperative (n=8), intraoperative (n=16) and postoperative (n=32) management, was conducted. The respondents included surgeons, anesthesiologists, and critical care specialists.</p><p><strong>Results: </strong>The response rate was 66% (136/206 clinicians contacted). Ninety-one percent of respondents reported implementing ERAS practices. There was encouraging adherence to implement the prehabilitation (76-95%), preoperative (50-94%), and intraoperative (55-90%) ERAS practices. Mechanical bowel preparation was being used by 84.5%. Intra-abdominal drains usage was 94.7%, intercostal drains by 77.9% respondents. Nasogastric drainage was used by 84% of practitioners. The average hospital stay was 10 days as reported by 50% of respondents. A working protocol and ERAS checklist have been designed, based on the results of our study, following recent ERAS-CRS-HIPEC guidelines. This protocol will be prospectively validated.</p><p><strong>Conclusions: </strong>Most respondents were implementing ERAS practices for patients undergoing CRS-HIPEC, though as an extrapolation of colorectal and gynecological guidelines. The adoption of postoperative practices was relatively low compared to other perioperative practices.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"6 3","pages":"99-111"},"PeriodicalIF":2.0000,"publicationDate":"2021-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1515/pp-2021-0117","citationCount":"6","resultStr":"{\"title\":\"Enhanced recovery after surgery (ERAS) in cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC): a cross-sectional survey.\",\"authors\":\"Geetu Bhandoria, Sohan Lal Solanki, Mrugank Bhavsar, Kalpana Balakrishnan, Cherukuri Bapuji, Nitin Bhorkar, Prashant Bhandarkar, Sameer Bhosale, Jigeeshu V Divatia, Anik Ghosh, Vikas Mahajan, Abraham Peedicayil, Praveen Nath, Snita Sinukumar, Robin Thambudorai, Ramakrishnan Ayloor Seshadri, Aditi Bhatt\",\"doi\":\"10.1515/pp-2021-0117\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Enhanced recovery after surgery (ERAS) protocols have been questioned in patients undergoing cytoreductive surgery (CRS) with/without hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal malignancies. This survey was performed to study clinicians' practice about ERAS in patients undergoing CRS-HIPEC.</p><p><strong>Methods: </strong>An online survey, comprising 76 questions on elements of prehabilitation (n=11), preoperative (n=8), intraoperative (n=16) and postoperative (n=32) management, was conducted. The respondents included surgeons, anesthesiologists, and critical care specialists.</p><p><strong>Results: </strong>The response rate was 66% (136/206 clinicians contacted). Ninety-one percent of respondents reported implementing ERAS practices. There was encouraging adherence to implement the prehabilitation (76-95%), preoperative (50-94%), and intraoperative (55-90%) ERAS practices. Mechanical bowel preparation was being used by 84.5%. Intra-abdominal drains usage was 94.7%, intercostal drains by 77.9% respondents. Nasogastric drainage was used by 84% of practitioners. The average hospital stay was 10 days as reported by 50% of respondents. A working protocol and ERAS checklist have been designed, based on the results of our study, following recent ERAS-CRS-HIPEC guidelines. This protocol will be prospectively validated.</p><p><strong>Conclusions: </strong>Most respondents were implementing ERAS practices for patients undergoing CRS-HIPEC, though as an extrapolation of colorectal and gynecological guidelines. The adoption of postoperative practices was relatively low compared to other perioperative practices.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"6 3\",\"pages\":\"99-111\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2021-06-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1515/pp-2021-0117\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2021-0117\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2021-0117","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Enhanced recovery after surgery (ERAS) in cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC): a cross-sectional survey.
Objectives: Enhanced recovery after surgery (ERAS) protocols have been questioned in patients undergoing cytoreductive surgery (CRS) with/without hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal malignancies. This survey was performed to study clinicians' practice about ERAS in patients undergoing CRS-HIPEC.
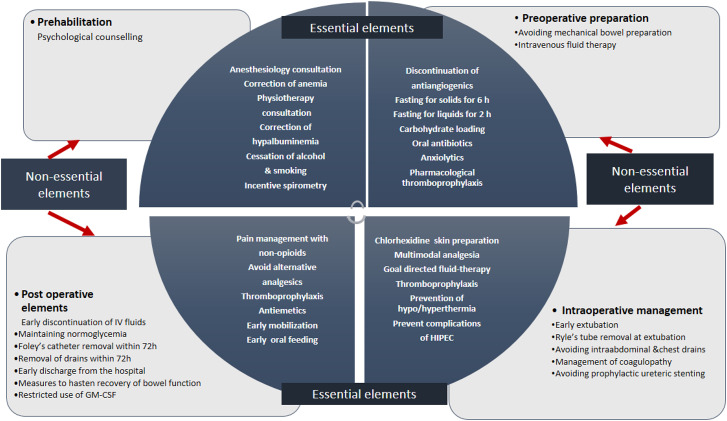
Methods: An online survey, comprising 76 questions on elements of prehabilitation (n=11), preoperative (n=8), intraoperative (n=16) and postoperative (n=32) management, was conducted. The respondents included surgeons, anesthesiologists, and critical care specialists.
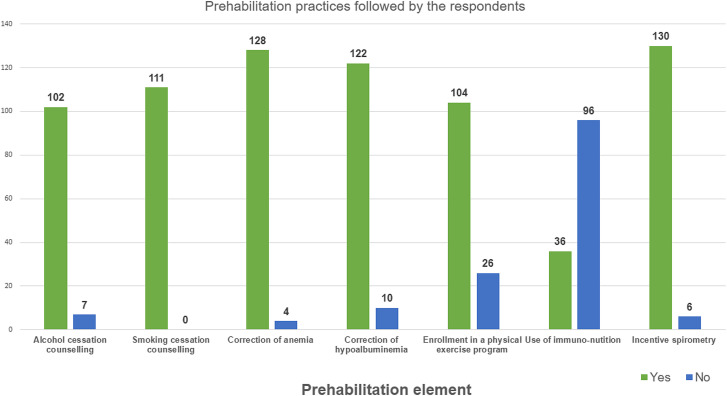
Results: The response rate was 66% (136/206 clinicians contacted). Ninety-one percent of respondents reported implementing ERAS practices. There was encouraging adherence to implement the prehabilitation (76-95%), preoperative (50-94%), and intraoperative (55-90%) ERAS practices. Mechanical bowel preparation was being used by 84.5%. Intra-abdominal drains usage was 94.7%, intercostal drains by 77.9% respondents. Nasogastric drainage was used by 84% of practitioners. The average hospital stay was 10 days as reported by 50% of respondents. A working protocol and ERAS checklist have been designed, based on the results of our study, following recent ERAS-CRS-HIPEC guidelines. This protocol will be prospectively validated.
Conclusions: Most respondents were implementing ERAS practices for patients undergoing CRS-HIPEC, though as an extrapolation of colorectal and gynecological guidelines. The adoption of postoperative practices was relatively low compared to other perioperative practices.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
