Minatallah A Elshafie, Magdy K Khalil, Maha L ElSheikh, Nagwa I Mowafy
{"title":"无阿片类药物麻醉用于肝硬化肝切除术患者的竖脊肌阻滞:一项随机对照试验。","authors":"Minatallah A Elshafie, Magdy K Khalil, Maha L ElSheikh, Nagwa I Mowafy","doi":"10.2147/LRA.S343347","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatic resection is a major abdominal surgery with challenging pain management. We aimed to investigate the effect of erector spinae plane block (ESPB) with opioid free anesthesia (OFA) in cirrhotic patients scheduled for liver resection on perioperative pain management in terms of hemodynamic stability. Secondarily, we assessed time to first request for analgesia and perioperative fentanyl consumption, nausea and vomiting within 24 hours after surgery.</p><p><strong>Methods: </strong>Forty patients were randomized to block group (n = 20): OFA with ESPB and conventional group (n = 20): conventional balanced anesthesia with opioids (OFA associated non-opioid drugs [dexmedetomidine, magnesium sulfate, xylocaine, and acetaminophen] and ESPB). Bilateral ESP block was done with ultrasound guidance at the level of thoracic vertebrae T 6-7, the local anesthetic dose was 20 mL Bupivacaine 0.25% with adjuvant dexmedetomidine (0.5 µg/kg) on each side. We monitored hemodynamic stability as the primary endpoint (heart rate, mean arterial blood pressure, and cardiac output).</p><p><strong>Results: </strong>Bilateral ESPB offered somatic and visceral analgesia for hepatic resection patients with no intraoperative fentanyl required. Postoperatively, the block group with dexmedetomidine adjuvant to the local anesthesia drugs showed delay in the first request for analgesia (<i>p</i> = 0.092) and decreased fentanyl requirement (<i>p</i> < 0.001), so no patient in the ESP group suffered from postoperative nausea and vomiting compared to 50% in the conventional group (<i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>Bilateral ESP block with OFA is an effective approach for intra- and postoperative analgesia in cirrhotic patients undergoing liver resection.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":" ","pages":"1-10"},"PeriodicalIF":1.9000,"publicationDate":"2022-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/cb/lra-15-1.PMC8801329.pdf","citationCount":"8","resultStr":"{\"title\":\"Erector Spinae Block with Opioid Free Anesthesia in Cirrhotic Patients Undergoing Hepatic Resection: A Randomized Controlled Trial.\",\"authors\":\"Minatallah A Elshafie, Magdy K Khalil, Maha L ElSheikh, Nagwa I Mowafy\",\"doi\":\"10.2147/LRA.S343347\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hepatic resection is a major abdominal surgery with challenging pain management. We aimed to investigate the effect of erector spinae plane block (ESPB) with opioid free anesthesia (OFA) in cirrhotic patients scheduled for liver resection on perioperative pain management in terms of hemodynamic stability. Secondarily, we assessed time to first request for analgesia and perioperative fentanyl consumption, nausea and vomiting within 24 hours after surgery.</p><p><strong>Methods: </strong>Forty patients were randomized to block group (n = 20): OFA with ESPB and conventional group (n = 20): conventional balanced anesthesia with opioids (OFA associated non-opioid drugs [dexmedetomidine, magnesium sulfate, xylocaine, and acetaminophen] and ESPB). Bilateral ESP block was done with ultrasound guidance at the level of thoracic vertebrae T 6-7, the local anesthetic dose was 20 mL Bupivacaine 0.25% with adjuvant dexmedetomidine (0.5 µg/kg) on each side. We monitored hemodynamic stability as the primary endpoint (heart rate, mean arterial blood pressure, and cardiac output).</p><p><strong>Results: </strong>Bilateral ESPB offered somatic and visceral analgesia for hepatic resection patients with no intraoperative fentanyl required. Postoperatively, the block group with dexmedetomidine adjuvant to the local anesthesia drugs showed delay in the first request for analgesia (<i>p</i> = 0.092) and decreased fentanyl requirement (<i>p</i> < 0.001), so no patient in the ESP group suffered from postoperative nausea and vomiting compared to 50% in the conventional group (<i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>Bilateral ESP block with OFA is an effective approach for intra- and postoperative analgesia in cirrhotic patients undergoing liver resection.</p>\",\"PeriodicalId\":18203,\"journal\":{\"name\":\"Local and Regional Anesthesia\",\"volume\":\" \",\"pages\":\"1-10\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2022-01-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/cb/lra-15-1.PMC8801329.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Local and Regional Anesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LRA.S343347\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S343347","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Erector Spinae Block with Opioid Free Anesthesia in Cirrhotic Patients Undergoing Hepatic Resection: A Randomized Controlled Trial.
Background: Hepatic resection is a major abdominal surgery with challenging pain management. We aimed to investigate the effect of erector spinae plane block (ESPB) with opioid free anesthesia (OFA) in cirrhotic patients scheduled for liver resection on perioperative pain management in terms of hemodynamic stability. Secondarily, we assessed time to first request for analgesia and perioperative fentanyl consumption, nausea and vomiting within 24 hours after surgery.
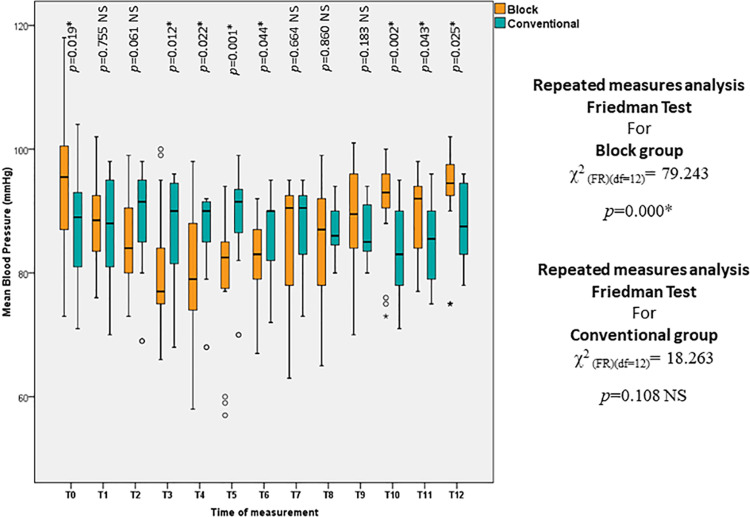
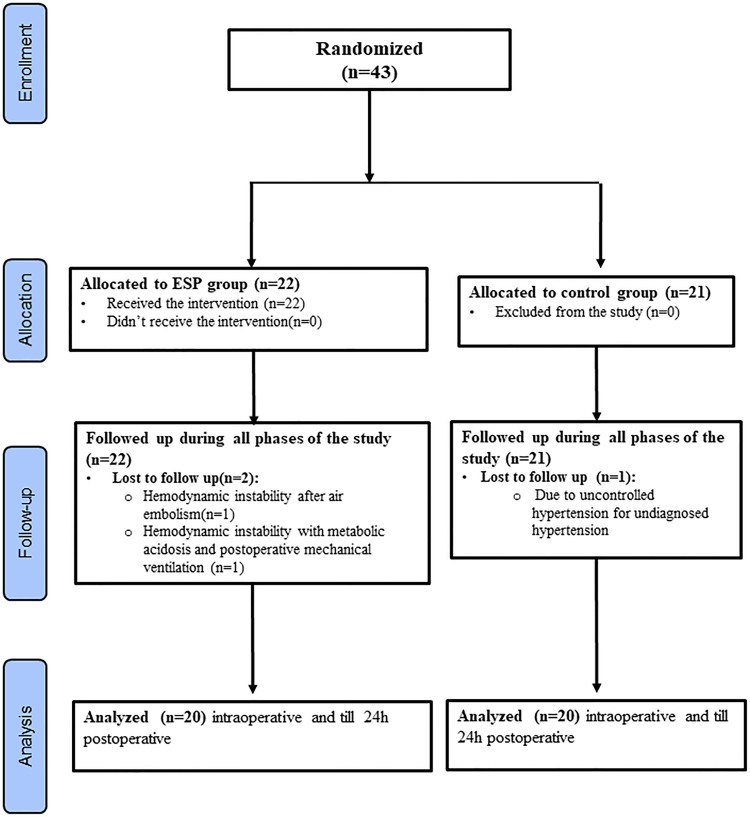
Methods: Forty patients were randomized to block group (n = 20): OFA with ESPB and conventional group (n = 20): conventional balanced anesthesia with opioids (OFA associated non-opioid drugs [dexmedetomidine, magnesium sulfate, xylocaine, and acetaminophen] and ESPB). Bilateral ESP block was done with ultrasound guidance at the level of thoracic vertebrae T 6-7, the local anesthetic dose was 20 mL Bupivacaine 0.25% with adjuvant dexmedetomidine (0.5 µg/kg) on each side. We monitored hemodynamic stability as the primary endpoint (heart rate, mean arterial blood pressure, and cardiac output).
Results: Bilateral ESPB offered somatic and visceral analgesia for hepatic resection patients with no intraoperative fentanyl required. Postoperatively, the block group with dexmedetomidine adjuvant to the local anesthesia drugs showed delay in the first request for analgesia (p = 0.092) and decreased fentanyl requirement (p < 0.001), so no patient in the ESP group suffered from postoperative nausea and vomiting compared to 50% in the conventional group (p < 0.001).
Conclusion: Bilateral ESP block with OFA is an effective approach for intra- and postoperative analgesia in cirrhotic patients undergoing liver resection.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
