Patrick Andersen, Anja Mizdrak, Nick Wilson, Anna Davies, Laxman Bablani, Tony Blakely
{"title":"按人口异质性分解比例多态生命表以估计干预对不平等的影响。","authors":"Patrick Andersen, Anja Mizdrak, Nick Wilson, Anna Davies, Laxman Bablani, Tony Blakely","doi":"10.1186/s12963-022-00282-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Simulation models can be used to quantify the projected health impact of interventions. Quantifying heterogeneity in these impacts, for example by socioeconomic status, is important to understand impacts on health inequalities. We aim to disaggregate one type of Markov macro-simulation model, the proportional multistate lifetable, ensuring that under business-as-usual (BAU) the sum of deaths across disaggregated strata in each time step returns the same as the initial non-disaggregated model. We then demonstrate the application by deprivation quintiles for New Zealand (NZ), for: hypothetical interventions (50% lower all-cause mortality, 50% lower coronary heart disease mortality) and a dietary intervention to substitute 59% of sodium with potassium chloride in the food supply.</p><p><strong>Methods: </strong>We developed a disaggregation algorithm that iteratively rescales mortality, incidence and case-fatality rates by time-step of the model to ensure correct total population counts were retained at each step. To demonstrate the algorithm on deprivation quintiles in NZ, we used the following inputs: overall (non-disaggregated) all-cause mortality & morbidity rates, coronary heart disease incidence & case fatality rates; stroke incidence & case fatality rates. We also obtained rate ratios by deprivation for these same measures. Given all-cause and cause-specific mortality rates by deprivation quintile, we derived values for the incidence, case fatality and mortality rates for each quintile, ensuring rate ratios across quintiles and the total population mortality and morbidity rates were returned when averaged across groups. The three interventions were then run on top of these scaled BAU scenarios.</p><p><strong>Results: </strong>The algorithm exactly disaggregated populations by strata in BAU. The intervention scenario life years and health adjusted life years (HALYs) gained differed slightly when summed over the deprivation quintile compared to the aggregated model, due to the stratified model (appropriately) allowing for differential background mortality rates by strata. Modest differences in health gains (HALYs) resulted from rescaling of sub-population mortality and incidence rates to ensure consistency with the aggregate population.</p><p><strong>Conclusion: </strong>Policy makers ideally need to know the effect of population interventions estimated both overall, and by socioeconomic and other strata. We demonstrate a method and provide code to do this routinely within proportional multistate lifetable simulation models and similar Markov models.</p>","PeriodicalId":3,"journal":{"name":"ACS Applied Electronic Materials","volume":" ","pages":"6"},"PeriodicalIF":4.7000,"publicationDate":"2022-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8761347/pdf/","citationCount":"1","resultStr":"{\"title\":\"Disaggregating proportional multistate lifetables by population heterogeneity to estimate intervention impacts on inequalities.\",\"authors\":\"Patrick Andersen, Anja Mizdrak, Nick Wilson, Anna Davies, Laxman Bablani, Tony Blakely\",\"doi\":\"10.1186/s12963-022-00282-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Simulation models can be used to quantify the projected health impact of interventions. Quantifying heterogeneity in these impacts, for example by socioeconomic status, is important to understand impacts on health inequalities. We aim to disaggregate one type of Markov macro-simulation model, the proportional multistate lifetable, ensuring that under business-as-usual (BAU) the sum of deaths across disaggregated strata in each time step returns the same as the initial non-disaggregated model. We then demonstrate the application by deprivation quintiles for New Zealand (NZ), for: hypothetical interventions (50% lower all-cause mortality, 50% lower coronary heart disease mortality) and a dietary intervention to substitute 59% of sodium with potassium chloride in the food supply.</p><p><strong>Methods: </strong>We developed a disaggregation algorithm that iteratively rescales mortality, incidence and case-fatality rates by time-step of the model to ensure correct total population counts were retained at each step. To demonstrate the algorithm on deprivation quintiles in NZ, we used the following inputs: overall (non-disaggregated) all-cause mortality & morbidity rates, coronary heart disease incidence & case fatality rates; stroke incidence & case fatality rates. We also obtained rate ratios by deprivation for these same measures. Given all-cause and cause-specific mortality rates by deprivation quintile, we derived values for the incidence, case fatality and mortality rates for each quintile, ensuring rate ratios across quintiles and the total population mortality and morbidity rates were returned when averaged across groups. The three interventions were then run on top of these scaled BAU scenarios.</p><p><strong>Results: </strong>The algorithm exactly disaggregated populations by strata in BAU. The intervention scenario life years and health adjusted life years (HALYs) gained differed slightly when summed over the deprivation quintile compared to the aggregated model, due to the stratified model (appropriately) allowing for differential background mortality rates by strata. Modest differences in health gains (HALYs) resulted from rescaling of sub-population mortality and incidence rates to ensure consistency with the aggregate population.</p><p><strong>Conclusion: </strong>Policy makers ideally need to know the effect of population interventions estimated both overall, and by socioeconomic and other strata. We demonstrate a method and provide code to do this routinely within proportional multistate lifetable simulation models and similar Markov models.</p>\",\"PeriodicalId\":3,\"journal\":{\"name\":\"ACS Applied Electronic Materials\",\"volume\":\" \",\"pages\":\"6\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2022-01-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8761347/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Electronic Materials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12963-022-00282-7\",\"RegionNum\":3,\"RegionCategory\":\"材料科学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENGINEERING, ELECTRICAL & ELECTRONIC\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Electronic Materials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12963-022-00282-7","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENGINEERING, ELECTRICAL & ELECTRONIC","Score":null,"Total":0}
Disaggregating proportional multistate lifetables by population heterogeneity to estimate intervention impacts on inequalities.
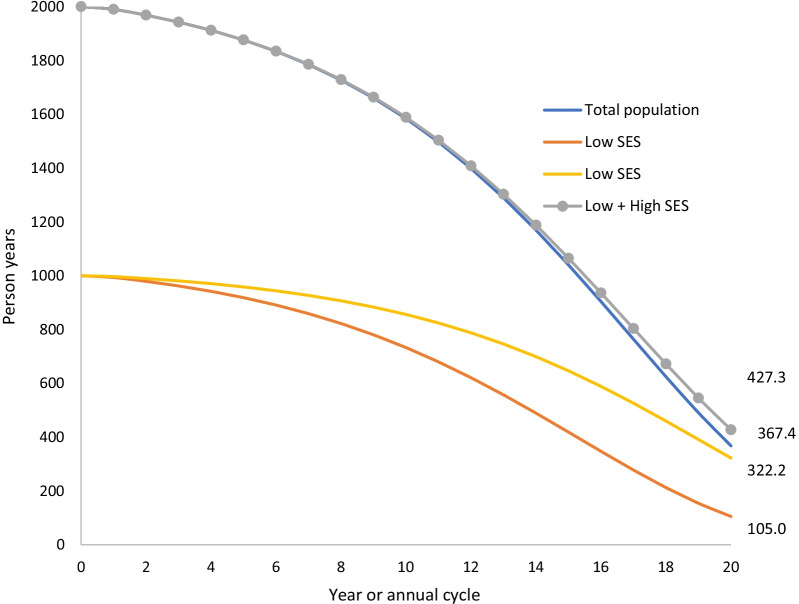
Background: Simulation models can be used to quantify the projected health impact of interventions. Quantifying heterogeneity in these impacts, for example by socioeconomic status, is important to understand impacts on health inequalities. We aim to disaggregate one type of Markov macro-simulation model, the proportional multistate lifetable, ensuring that under business-as-usual (BAU) the sum of deaths across disaggregated strata in each time step returns the same as the initial non-disaggregated model. We then demonstrate the application by deprivation quintiles for New Zealand (NZ), for: hypothetical interventions (50% lower all-cause mortality, 50% lower coronary heart disease mortality) and a dietary intervention to substitute 59% of sodium with potassium chloride in the food supply.
Methods: We developed a disaggregation algorithm that iteratively rescales mortality, incidence and case-fatality rates by time-step of the model to ensure correct total population counts were retained at each step. To demonstrate the algorithm on deprivation quintiles in NZ, we used the following inputs: overall (non-disaggregated) all-cause mortality & morbidity rates, coronary heart disease incidence & case fatality rates; stroke incidence & case fatality rates. We also obtained rate ratios by deprivation for these same measures. Given all-cause and cause-specific mortality rates by deprivation quintile, we derived values for the incidence, case fatality and mortality rates for each quintile, ensuring rate ratios across quintiles and the total population mortality and morbidity rates were returned when averaged across groups. The three interventions were then run on top of these scaled BAU scenarios.
Results: The algorithm exactly disaggregated populations by strata in BAU. The intervention scenario life years and health adjusted life years (HALYs) gained differed slightly when summed over the deprivation quintile compared to the aggregated model, due to the stratified model (appropriately) allowing for differential background mortality rates by strata. Modest differences in health gains (HALYs) resulted from rescaling of sub-population mortality and incidence rates to ensure consistency with the aggregate population.
Conclusion: Policy makers ideally need to know the effect of population interventions estimated both overall, and by socioeconomic and other strata. We demonstrate a method and provide code to do this routinely within proportional multistate lifetable simulation models and similar Markov models.
期刊介绍:
ACS Applied Electronic Materials is an interdisciplinary journal publishing original research covering all aspects of electronic materials. The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrate knowledge in the areas of materials science, engineering, optics, physics, and chemistry into important applications of electronic materials. Sample research topics that span the journal's scope are inorganic, organic, ionic and polymeric materials with properties that include conducting, semiconducting, superconducting, insulating, dielectric, magnetic, optoelectronic, piezoelectric, ferroelectric and thermoelectric.
Indexed/Abstracted:
Web of Science SCIE
Scopus
CAS
INSPEC
Portico



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
