Stavros Matsoukas, Brian Giovanni, Liorah Rubinstein, Shahram Majidi, Laura K Stein, Johanna T Fifi
{"title":"模拟院前分诊对真实生活点滴和船舶机械取栓的城市患者队列的影响。","authors":"Stavros Matsoukas, Brian Giovanni, Liorah Rubinstein, Shahram Majidi, Laura K Stein, Johanna T Fifi","doi":"10.1159/000520078","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of the study was to model the effect of prehospital triage of emergent large vessel occlusion (ELVO) to endovascular capable center (ECC) on the timing of thrombectomy and intravenous (IV) thrombolysis using real-world data from a multihospital system.</p><p><strong>Methods: </strong>We selected a cohort of 77 consecutive stroke patients who were brought by emergency medical services (EMS) to a nonendovascular capable center and then transferred to an ECC for mechanical thrombectomy (MT) (\"actual\" drip and ship [DS] cohort). We created a hypothetical scenario (bypass model [BM]), modeling transfer of the patients directly to an ECC, based on patients' initial EMS pickup address and closest ECC. Using another cohort of 73 consecutive patients, who were brought directly to an ECC by EMS and underwent endovascular intervention, we calculated mean door-to-needle and door-to-arterial puncture (AP) times (\"actual\" mothership [MS] cohort). Timings in the actual MS cohort and the actual DS cohort were compared to timings from the BM cohort.</p><p><strong>Results: </strong>Median first medical contact (FMC) to IV thrombolysis time was 87.5 min (interquartile range [IQR] = 38) for the DS versus 78.5 min (IQR = 8.96) for the BM cohort, with p = 0.1672. Median FMC to AP was 244 min (IQR = 97) versus 147 min (IQR = 8.96) (p < 0.001), and median FMC to TICI 2B+ time was 299 min (IQR = 108.5) versus 197 min (IQR = 8.96) (p < 0.001) for the DS versus BM cohort, respectively.</p><p><strong>Conclusions: </strong>Modeled EMS prehospital triage of ELVO patients' results in shorter MT times without a change in thrombolysis times. As triage tools increase in sensitivity and specificity, EMS triage protocols stand to improve patient outcomes.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":"11 3","pages":"137-144"},"PeriodicalIF":2.1000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/30/cee-0011-0137.PMC8740215.pdf","citationCount":"0","resultStr":"{\"title\":\"Modeling the Impact of Prehospital Triage on a True-Life Drip and Ship Mechanical Thrombectomy Urban Patient Cohort.\",\"authors\":\"Stavros Matsoukas, Brian Giovanni, Liorah Rubinstein, Shahram Majidi, Laura K Stein, Johanna T Fifi\",\"doi\":\"10.1159/000520078\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The aim of the study was to model the effect of prehospital triage of emergent large vessel occlusion (ELVO) to endovascular capable center (ECC) on the timing of thrombectomy and intravenous (IV) thrombolysis using real-world data from a multihospital system.</p><p><strong>Methods: </strong>We selected a cohort of 77 consecutive stroke patients who were brought by emergency medical services (EMS) to a nonendovascular capable center and then transferred to an ECC for mechanical thrombectomy (MT) (\\\"actual\\\" drip and ship [DS] cohort). We created a hypothetical scenario (bypass model [BM]), modeling transfer of the patients directly to an ECC, based on patients' initial EMS pickup address and closest ECC. Using another cohort of 73 consecutive patients, who were brought directly to an ECC by EMS and underwent endovascular intervention, we calculated mean door-to-needle and door-to-arterial puncture (AP) times (\\\"actual\\\" mothership [MS] cohort). Timings in the actual MS cohort and the actual DS cohort were compared to timings from the BM cohort.</p><p><strong>Results: </strong>Median first medical contact (FMC) to IV thrombolysis time was 87.5 min (interquartile range [IQR] = 38) for the DS versus 78.5 min (IQR = 8.96) for the BM cohort, with p = 0.1672. Median FMC to AP was 244 min (IQR = 97) versus 147 min (IQR = 8.96) (p < 0.001), and median FMC to TICI 2B+ time was 299 min (IQR = 108.5) versus 197 min (IQR = 8.96) (p < 0.001) for the DS versus BM cohort, respectively.</p><p><strong>Conclusions: </strong>Modeled EMS prehospital triage of ELVO patients' results in shorter MT times without a change in thrombolysis times. As triage tools increase in sensitivity and specificity, EMS triage protocols stand to improve patient outcomes.</p>\",\"PeriodicalId\":45709,\"journal\":{\"name\":\"Cerebrovascular Diseases Extra\",\"volume\":\"11 3\",\"pages\":\"137-144\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/30/cee-0011-0137.PMC8740215.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000520078\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/11/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000520078","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/11/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Modeling the Impact of Prehospital Triage on a True-Life Drip and Ship Mechanical Thrombectomy Urban Patient Cohort.
Objective: The aim of the study was to model the effect of prehospital triage of emergent large vessel occlusion (ELVO) to endovascular capable center (ECC) on the timing of thrombectomy and intravenous (IV) thrombolysis using real-world data from a multihospital system.
Methods: We selected a cohort of 77 consecutive stroke patients who were brought by emergency medical services (EMS) to a nonendovascular capable center and then transferred to an ECC for mechanical thrombectomy (MT) ("actual" drip and ship [DS] cohort). We created a hypothetical scenario (bypass model [BM]), modeling transfer of the patients directly to an ECC, based on patients' initial EMS pickup address and closest ECC. Using another cohort of 73 consecutive patients, who were brought directly to an ECC by EMS and underwent endovascular intervention, we calculated mean door-to-needle and door-to-arterial puncture (AP) times ("actual" mothership [MS] cohort). Timings in the actual MS cohort and the actual DS cohort were compared to timings from the BM cohort.
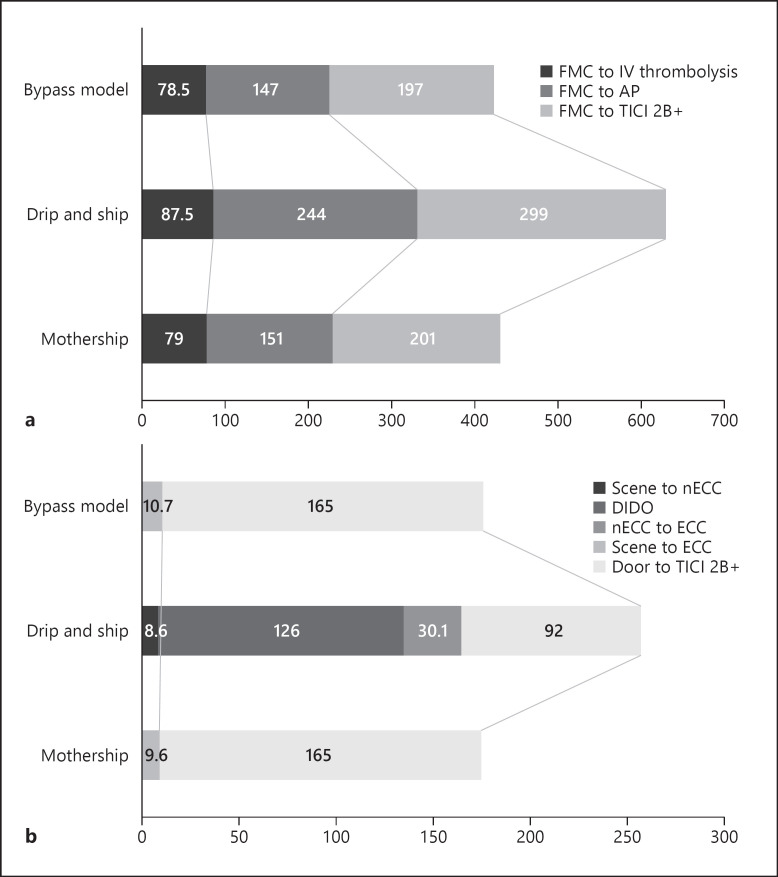
Results: Median first medical contact (FMC) to IV thrombolysis time was 87.5 min (interquartile range [IQR] = 38) for the DS versus 78.5 min (IQR = 8.96) for the BM cohort, with p = 0.1672. Median FMC to AP was 244 min (IQR = 97) versus 147 min (IQR = 8.96) (p < 0.001), and median FMC to TICI 2B+ time was 299 min (IQR = 108.5) versus 197 min (IQR = 8.96) (p < 0.001) for the DS versus BM cohort, respectively.
Conclusions: Modeled EMS prehospital triage of ELVO patients' results in shorter MT times without a change in thrombolysis times. As triage tools increase in sensitivity and specificity, EMS triage protocols stand to improve patient outcomes.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
