Justin Lin, Yue Zhang, Wei Hou, Qian Qin, Matthew D Galsky, William K Oh, Che-Kai Tsao
{"title":"肾细胞癌转移模式的演变:我们是否需要进行常规骨成像?","authors":"Justin Lin, Yue Zhang, Wei Hou, Qian Qin, Matthew D Galsky, William K Oh, Che-Kai Tsao","doi":"10.15586/jkcvhl.v8i4.202","DOIUrl":null,"url":null,"abstract":"<p><p>Advance diagnostic and treatment modalities have improved outcomes for renal cell carcinoma (RCC) patients, but the prognosis for those with metastatic disease (mRCC) remains poor. As given metastatic distribution is critical in guiding treatment decisions for mRCC patients, we evaluated evolving metastatic patterns to assess if our current practice standards effectively address patient needs. A systematic literature review was performed to identify all publicly available prospective clinical trials in metastatic renal cell carcinoma (mRCC) from 1990 to 2018. A total of 16,899 mRCC patients from 127 qualified phase I-III clinical trials with metastatic site documentations were included for analysis for incidence of metastases to lung, liver, bone, and lymph nodes (LNs) over time. Studies were categorized into three treatment eras based on the timing of regulatory approval: Cytokine Era (1990-2004), vascular endothelial growth factor/tyrosine kinase inhibitor (TKI) Era (2005-2016), and immune checkpoint inhibitor/TKI Era (ICI-TKI, 2017-2018) and also classified as first-line only (FLO) or second-line and beyond (SLB). Overall, an increase in the incidence of bone and LNs metastases in FLO and SLB, and lung metastases in FLO, was seen over the three treatment eras. Generally, the burden of disease is higher in SLB when compared with FLO. Importantly, in the ICI-TKI era, the incidences of bone metastasis are 28% in FLO and 29% in SLB settings. The disease burden in patients with mRCC has increased steadily over the past three decades. Given the unexpectedly high rate of bone metastasis, routine dedicated bone imaging should be considered in all patients with mRCC.</p>","PeriodicalId":44291,"journal":{"name":"Journal of Kidney Cancer and VHL","volume":"8 4","pages":"13-19"},"PeriodicalIF":1.9000,"publicationDate":"2021-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8523177/pdf/","citationCount":"2","resultStr":"{\"title\":\"Evolving Patterns of Metastasis in Renal Cell Carcinoma: Do We Need to Perform Routine Bone Imaging?\",\"authors\":\"Justin Lin, Yue Zhang, Wei Hou, Qian Qin, Matthew D Galsky, William K Oh, Che-Kai Tsao\",\"doi\":\"10.15586/jkcvhl.v8i4.202\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Advance diagnostic and treatment modalities have improved outcomes for renal cell carcinoma (RCC) patients, but the prognosis for those with metastatic disease (mRCC) remains poor. As given metastatic distribution is critical in guiding treatment decisions for mRCC patients, we evaluated evolving metastatic patterns to assess if our current practice standards effectively address patient needs. A systematic literature review was performed to identify all publicly available prospective clinical trials in metastatic renal cell carcinoma (mRCC) from 1990 to 2018. A total of 16,899 mRCC patients from 127 qualified phase I-III clinical trials with metastatic site documentations were included for analysis for incidence of metastases to lung, liver, bone, and lymph nodes (LNs) over time. Studies were categorized into three treatment eras based on the timing of regulatory approval: Cytokine Era (1990-2004), vascular endothelial growth factor/tyrosine kinase inhibitor (TKI) Era (2005-2016), and immune checkpoint inhibitor/TKI Era (ICI-TKI, 2017-2018) and also classified as first-line only (FLO) or second-line and beyond (SLB). Overall, an increase in the incidence of bone and LNs metastases in FLO and SLB, and lung metastases in FLO, was seen over the three treatment eras. Generally, the burden of disease is higher in SLB when compared with FLO. Importantly, in the ICI-TKI era, the incidences of bone metastasis are 28% in FLO and 29% in SLB settings. The disease burden in patients with mRCC has increased steadily over the past three decades. Given the unexpectedly high rate of bone metastasis, routine dedicated bone imaging should be considered in all patients with mRCC.</p>\",\"PeriodicalId\":44291,\"journal\":{\"name\":\"Journal of Kidney Cancer and VHL\",\"volume\":\"8 4\",\"pages\":\"13-19\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2021-10-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8523177/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Kidney Cancer and VHL\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15586/jkcvhl.v8i4.202\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Kidney Cancer and VHL","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15586/jkcvhl.v8i4.202","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Evolving Patterns of Metastasis in Renal Cell Carcinoma: Do We Need to Perform Routine Bone Imaging?
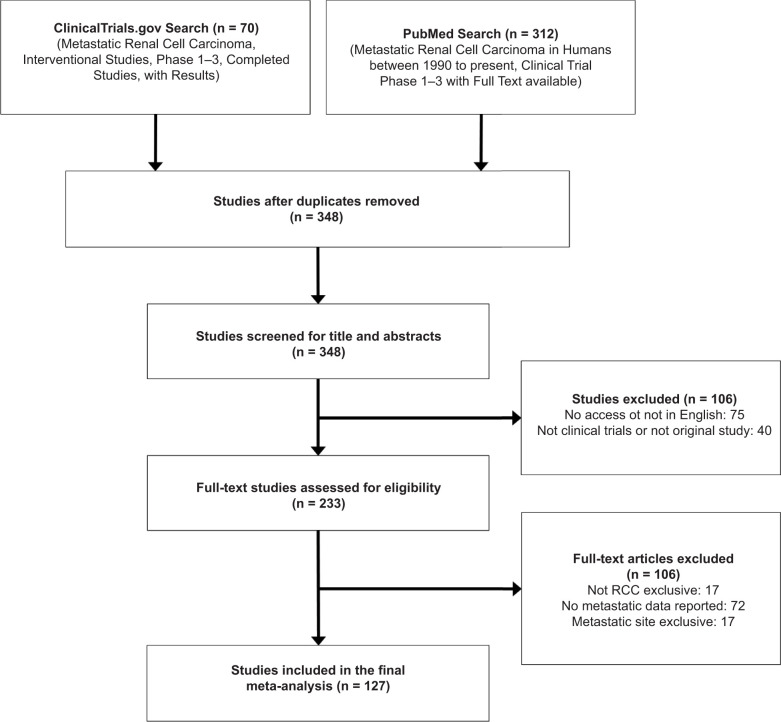
Advance diagnostic and treatment modalities have improved outcomes for renal cell carcinoma (RCC) patients, but the prognosis for those with metastatic disease (mRCC) remains poor. As given metastatic distribution is critical in guiding treatment decisions for mRCC patients, we evaluated evolving metastatic patterns to assess if our current practice standards effectively address patient needs. A systematic literature review was performed to identify all publicly available prospective clinical trials in metastatic renal cell carcinoma (mRCC) from 1990 to 2018. A total of 16,899 mRCC patients from 127 qualified phase I-III clinical trials with metastatic site documentations were included for analysis for incidence of metastases to lung, liver, bone, and lymph nodes (LNs) over time. Studies were categorized into three treatment eras based on the timing of regulatory approval: Cytokine Era (1990-2004), vascular endothelial growth factor/tyrosine kinase inhibitor (TKI) Era (2005-2016), and immune checkpoint inhibitor/TKI Era (ICI-TKI, 2017-2018) and also classified as first-line only (FLO) or second-line and beyond (SLB). Overall, an increase in the incidence of bone and LNs metastases in FLO and SLB, and lung metastases in FLO, was seen over the three treatment eras. Generally, the burden of disease is higher in SLB when compared with FLO. Importantly, in the ICI-TKI era, the incidences of bone metastasis are 28% in FLO and 29% in SLB settings. The disease burden in patients with mRCC has increased steadily over the past three decades. Given the unexpectedly high rate of bone metastasis, routine dedicated bone imaging should be considered in all patients with mRCC.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
