{"title":"多胎与单胎的比较:多中心KID数据库的分析。","authors":"Renjithkumar Kalikkot Thekkeveedu, Nilesh Dankhara, Jagdish Desai, Angelle L Klar, Jaimin Patel","doi":"10.1186/s40748-021-00135-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The available data regarding morbidity and mortality associated with multiple gestation births is conflicting and contradicting.</p><p><strong>Objective: </strong>To compare morbidity, mortality, and length of stay (LOS) outcomes between multiple gestation (twin, triplet and higher-order) and singleton births.</p><p><strong>Methods: </strong>Data from the national multicenter Kids' Inpatient Database of the Healthcare Cost and Utilization Project from the years 2000, 2003, 2006, 2009, 2012, and 2016 were analyzed using a complex survey design using Statistical Analysis System (SAS) 9.4 (SAS Institute, Cary NC). Neonates with ICD9 and ICD10 codes indicating singletons, twins or triplets, and higher-order multiples were included. Mortality was compared between these groups after excluding transfer outs to avoid duplicate inclusion. To analyze LOS, we included inborn neonates and excluded transfers; who died inpatient and any neonates who appear to have been discharged less than 33 weeks PMA. The LOS was compared by gestational age groups.</p><p><strong>Results: </strong>A total of 22,853,125 neonates were analyzed for mortality after applying inclusion-exclusion criteria; 2.96% were twins, and 0.13% were triplets or more. A total of 22,690,082 neonates were analyzed for LOS. Mean GA, expressed as mean (SD), for singleton, twins and triplets, were 38.30 (2.21), 36.39 (4.21), and 32.72 (4.14), respectively. The adjusted odds for mortality were similar for twin births compared to singleton (aOR: 1.004, 95% CI:0.960-1.051, p = 0.8521). The adjusted odds of mortality for triplet or higher-order gestation births were higher (aOR: 1.33, 95% CI: 1.128-1.575, p = 0.0008) when compared to the singleton births. Median LOS (days) was significantly longer in multiple gestation compared to singleton births overall (singletons: 1.59 [1.13, 2.19] vs. twins 3.29 [2.17, 9.59] vs. triplets or higher-order multiples 19.15 [8.80, 36.38], p < .0001), and this difference remained significant within each GA category.</p><p><strong>Conclusion: </strong>Multiple gestation births have higher mortality and longer LOS when compared to singleton births. This population data from multiple centers across the country could be useful in counseling parents when caring for multiple gestation pregnancies.</p>","PeriodicalId":74120,"journal":{"name":"Maternal health, neonatology and perinatology","volume":" ","pages":"15"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8554969/pdf/","citationCount":"22","resultStr":"{\"title\":\"Outcomes of multiple gestation births compared to singleton: analysis of multicenter KID database.\",\"authors\":\"Renjithkumar Kalikkot Thekkeveedu, Nilesh Dankhara, Jagdish Desai, Angelle L Klar, Jaimin Patel\",\"doi\":\"10.1186/s40748-021-00135-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The available data regarding morbidity and mortality associated with multiple gestation births is conflicting and contradicting.</p><p><strong>Objective: </strong>To compare morbidity, mortality, and length of stay (LOS) outcomes between multiple gestation (twin, triplet and higher-order) and singleton births.</p><p><strong>Methods: </strong>Data from the national multicenter Kids' Inpatient Database of the Healthcare Cost and Utilization Project from the years 2000, 2003, 2006, 2009, 2012, and 2016 were analyzed using a complex survey design using Statistical Analysis System (SAS) 9.4 (SAS Institute, Cary NC). Neonates with ICD9 and ICD10 codes indicating singletons, twins or triplets, and higher-order multiples were included. Mortality was compared between these groups after excluding transfer outs to avoid duplicate inclusion. To analyze LOS, we included inborn neonates and excluded transfers; who died inpatient and any neonates who appear to have been discharged less than 33 weeks PMA. The LOS was compared by gestational age groups.</p><p><strong>Results: </strong>A total of 22,853,125 neonates were analyzed for mortality after applying inclusion-exclusion criteria; 2.96% were twins, and 0.13% were triplets or more. A total of 22,690,082 neonates were analyzed for LOS. Mean GA, expressed as mean (SD), for singleton, twins and triplets, were 38.30 (2.21), 36.39 (4.21), and 32.72 (4.14), respectively. The adjusted odds for mortality were similar for twin births compared to singleton (aOR: 1.004, 95% CI:0.960-1.051, p = 0.8521). The adjusted odds of mortality for triplet or higher-order gestation births were higher (aOR: 1.33, 95% CI: 1.128-1.575, p = 0.0008) when compared to the singleton births. Median LOS (days) was significantly longer in multiple gestation compared to singleton births overall (singletons: 1.59 [1.13, 2.19] vs. twins 3.29 [2.17, 9.59] vs. triplets or higher-order multiples 19.15 [8.80, 36.38], p < .0001), and this difference remained significant within each GA category.</p><p><strong>Conclusion: </strong>Multiple gestation births have higher mortality and longer LOS when compared to singleton births. This population data from multiple centers across the country could be useful in counseling parents when caring for multiple gestation pregnancies.</p>\",\"PeriodicalId\":74120,\"journal\":{\"name\":\"Maternal health, neonatology and perinatology\",\"volume\":\" \",\"pages\":\"15\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-10-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8554969/pdf/\",\"citationCount\":\"22\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Maternal health, neonatology and perinatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40748-021-00135-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maternal health, neonatology and perinatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40748-021-00135-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 22
摘要
背景:关于多胎妊娠相关的发病率和死亡率的现有数据是相互矛盾的。目的:比较多胎妊娠(双胎、三胞胎和高胎)和单胎妊娠的发病率、死亡率和住院时间(LOS)。方法:采用SAS 9.4统计分析系统(SAS Institute, Cary NC)对2000年、2003年、2006年、2009年、2012年和2016年全国多中心儿童住院医疗费用与利用项目数据库数据进行复杂调查设计分析。新生儿的ICD9和ICD10代码表示单胎,双胞胎或三胞胎,以及高阶倍数。在排除转移以避免重复纳入后,比较两组之间的死亡率。为了分析LOS,我们纳入了出生的新生儿,排除了转移;在住院期间死亡的婴儿和出院时间少于33周的新生儿。对不同胎龄组的LOS进行比较。结果:采用纳入-排除标准,共分析了22,853,125例新生儿的死亡率;2.96%是双胞胎,0.13%是三胞胎或更多。共对22,690,082名新生儿进行了LOS分析。单胎、双胞胎和三胞胎的平均GA分别为38.30(2.21)、36.39(4.21)和32.72(4.14)。双胞胎与单胎的调整后死亡率相似(aOR: 1.004, 95% CI:0.960-1.051, p = 0.8521)。与单胎分娩相比,三胞胎或高阶妊娠分娩的调整后死亡率更高(aOR: 1.33, 95% CI: 1.128-1.575, p = 0.0008)。与单胎分娩相比,多胎妊娠的平均LOS(天)明显更长(单胎:1.59[1.13,2.19],双胞胎:3.29[2.17,9.59],三胞胎或高次胎19.15 [8.80,36.38],p结论:与单胎分娩相比,多胎妊娠分娩死亡率更高,LOS更长。来自全国多个中心的人口数据可以在照顾多胎妊娠时为父母提供有用的咨询。
Outcomes of multiple gestation births compared to singleton: analysis of multicenter KID database.
Background: The available data regarding morbidity and mortality associated with multiple gestation births is conflicting and contradicting.
Objective: To compare morbidity, mortality, and length of stay (LOS) outcomes between multiple gestation (twin, triplet and higher-order) and singleton births.
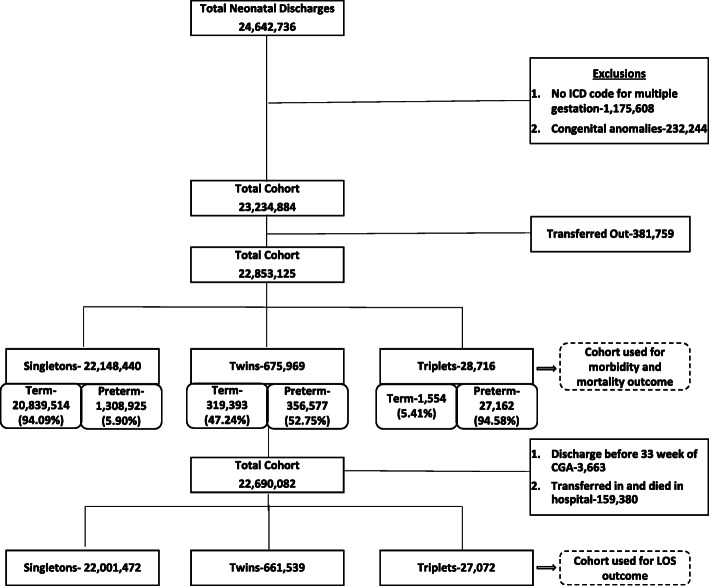
Methods: Data from the national multicenter Kids' Inpatient Database of the Healthcare Cost and Utilization Project from the years 2000, 2003, 2006, 2009, 2012, and 2016 were analyzed using a complex survey design using Statistical Analysis System (SAS) 9.4 (SAS Institute, Cary NC). Neonates with ICD9 and ICD10 codes indicating singletons, twins or triplets, and higher-order multiples were included. Mortality was compared between these groups after excluding transfer outs to avoid duplicate inclusion. To analyze LOS, we included inborn neonates and excluded transfers; who died inpatient and any neonates who appear to have been discharged less than 33 weeks PMA. The LOS was compared by gestational age groups.
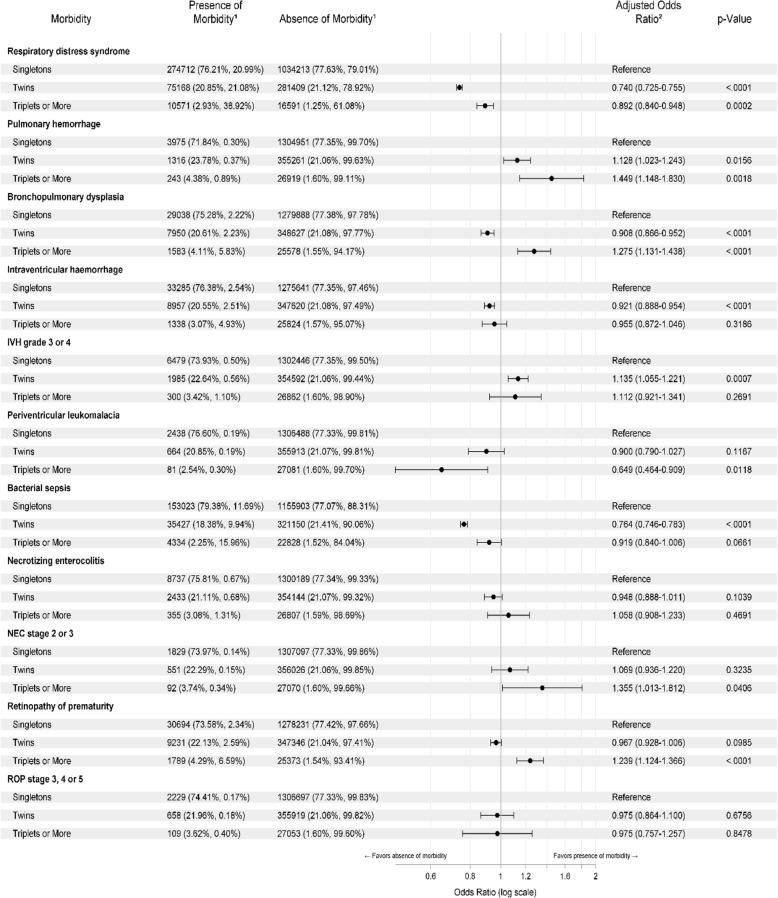
Results: A total of 22,853,125 neonates were analyzed for mortality after applying inclusion-exclusion criteria; 2.96% were twins, and 0.13% were triplets or more. A total of 22,690,082 neonates were analyzed for LOS. Mean GA, expressed as mean (SD), for singleton, twins and triplets, were 38.30 (2.21), 36.39 (4.21), and 32.72 (4.14), respectively. The adjusted odds for mortality were similar for twin births compared to singleton (aOR: 1.004, 95% CI:0.960-1.051, p = 0.8521). The adjusted odds of mortality for triplet or higher-order gestation births were higher (aOR: 1.33, 95% CI: 1.128-1.575, p = 0.0008) when compared to the singleton births. Median LOS (days) was significantly longer in multiple gestation compared to singleton births overall (singletons: 1.59 [1.13, 2.19] vs. twins 3.29 [2.17, 9.59] vs. triplets or higher-order multiples 19.15 [8.80, 36.38], p < .0001), and this difference remained significant within each GA category.
Conclusion: Multiple gestation births have higher mortality and longer LOS when compared to singleton births. This population data from multiple centers across the country could be useful in counseling parents when caring for multiple gestation pregnancies.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
